
Actoplus Met
General Information about Actoplus Met
Type 2 diabetes is a persistent condition that impacts hundreds of thousands of people worldwide. It happens when the physique is unable to supply enough insulin or turns into immune to insulin, resulting in excessive blood sugar levels. If left untreated, kind 2 diabetes can lead to critical problems similar to coronary heart disease, stroke, nerve harm, and kidney failure. Therefore, it's important to successfully manage blood sugar levels to prevent these complications.
Another benefit of Actoplus Met is that it may additionally help to decrease blood pressure and decrease harmful levels of cholesterol. This makes it a useful possibility for patients with kind 2 diabetes who also have hypertension or excessive cholesterol. Actoplus Met can also be well-tolerated by most patients and has a considerably decrease threat of hypoglycemia (low blood sugar) compared to other drugs used to treat diabetes.
In conclusion, Actoplus Met is a popular and efficient medicine for the treatment of type 2 diabetes. Its twin action mechanism helps regulate blood sugar ranges and may also present further benefits corresponding to decreasing blood stress and cholesterol levels. However, as with every medicine, it's important to comply with the prescribed dosage and report any regarding signs to a healthcare supplier. With the correct use of Actoplus Met, individuals with type 2 diabetes can better handle their situation and enhance their total health.
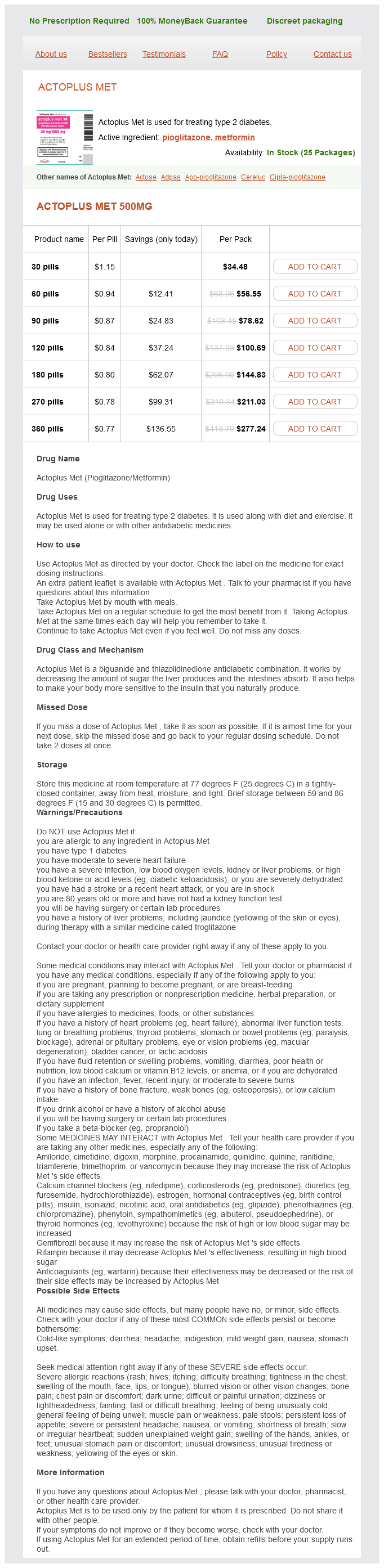
Actoplus Met is a medicine that's commonly prescribed for the remedy of kind 2 diabetes. It is a combination of two completely different medication - pioglitazone and metformin. This combination works by serving to the physique use insulin extra effectively and by lowering the amount of sugar produced by the liver. Actoplus Met is usually used in conjunction with a healthy diet and train to assist handle blood sugar ranges in sufferers with type 2 diabetes.
One of the first advantages of Actoplus Met is its ability to successfully lower blood sugar levels. Pioglitazone works by increasing the physique's sensitivity to insulin, whereas metformin reduces the quantity of sugar produced by the liver and improves the muscle's capacity to soak up glucose. This twin motion helps regulate blood sugar ranges and prevents them from turning into too excessive.
As with any medication, there are potential unwanted facet effects related to Actoplus Met. The most typical unwanted effects embody nausea, vomiting, diarrhea, dizziness, and headache. Some patients may experience weight gain or fluid retention. However, these unwanted effects are gentle and usually go away on their own. In uncommon instances, Actoplus Met might trigger more severe side effects, corresponding to liver issues or heart failure. It is important to report any new or regarding signs to a healthcare provider instantly.
Actoplus Met is a once-daily treatment that comes within the type of a tablet. It is often taken with meals to reduce the risk of stomach upset. The dosage of Actoplus Met might vary and is determined by a healthcare provider based on factors such as the affected person's age, weight, and response to the medicine. Typically, the beginning dose is 15mg of pioglitazone and 500mg of metformin, which can be adjusted as needed.
Rhinomanometry Technique Nasal airflow is best measured using a face mask that is large enough that it does not distort the external nasal structures diabetes medications generic names buy generic actoplus met 500 mg. For pressure detection, silastic tubing is secured by tape to the side of the nose not being measured. The patient is given the mask to hold, and then is instructed to put it on his or her face with the chin in the appropriate location and to take several breaths with the mouth closed. This relieves any apprehension about wearing the mask and also verifies an appropriate fit. If the machine requires a baseline collection (similar to adjusting a digital bathroom scale to zero) this is done before any connection to the device. The appropriately shaped tape to cover the left nostril is fastened to the pressure tube that comes into the inside of the mask. This in turn is attached to the left nostril for pressure detection to the nasopharynx while leaving the right nostril open for testing. The pressure-flow curve is visualized on the computer display and any needed adjustments are made. Transnasal pressure is measured between the pressure in the mask and the pressure in the nasopharynx detected through a tube attached to the opposite nostril. The curvature is due to smaller increases in flow (y-axis) for each increase in pressure at points farther from the origin. Resistance (pressure divided by flow) values therefore increase at more distal points on the pressure-flow curve because of this nonlinear relationship. Various parameters can be calculated from the pressure and flow data that were stored by the computer. Using this parameter from both the right and left sides of the airway, the total nasal airflow at 150 Pa may be calculated by adding the two flows that were obtained at the same pressure. Another important parameter is the resistance at the peak pressure and flow point called the maximum resistance1,8,9 or the vertex resistance by Vogt. This parameter was also found to correlate best with the symptom of nasal obstruction when compared with a wide array of other proposed parameters. If testing is not going to be done with dilators but is going to be done after decongestion, application of a decongestant spray. If testing will be done with dilating plastic strips or other dilating devices, these are placed and the previously listed procedures are repeated for both sides of the nose. If testing will be done following both dilation and nasal decongestion, testing with dilation alone precedes the testing with dilation and decongestion so that the dilating strips will remain in a consistent position. For children, a smaller face mask can be used, but the test is performed in the same way as for adults. For patients whose chief complaint is nasal obstruction when recumbent, additional studies can be performed in the supine, right-side lying, and left-side lying positions, preferably with appropriate delay after positioning before testing. For patients with suspected allergic rhinitis, nasal provocation testing can be performed. Sources of Variability It is important to understand potential causes of variability in rhinomanometry. If the patient laughs, speaks, or opens his or her mouth during the test, then it will cause an error in the recording. In many patients, this would be minimal because the alar muscles tend to work toward stabilization of the vestibular wall. Some variability has been attributed to mask use, but in general, masks distort the alae much less than do nozzles, and different mask shapes and volumes do not significantly affect rhinomanometric measurements. To minimize the variability while performing a rhinomanometry, the apparatus should first be at room temperature and then should be properly calibrated. The mask, which is preferred to nozzles, should fit without an air leak throughout the test. It is best to view the display of the pressure-flow curve in real time so that mask leaks or Reporting Results One way to evaluate the results of the test is to examine the pressure-flow curve. A flattening of the curve may represent flow limitation from an airway restriction. Looping of the 72 Rhinology other artifacts may be detected and addressed during the exam. The patient should be instructed to keep his or her mouth closed and to not speak during the test. Acoustic Rhinometry Technique the equipment used in acoustic rhinometry has been described by Hilberg et al. Variations in the cross-sectional area of the nose affect the reflectance of the sound. A microphone detects the reflected sound, and the signal from the microphone is processed and then converted to digital data. A computer then calculates and plots an area-distance function from the data, yielding a profile of the cross-sectional areas through each side of the nose. Surgical lubricant is used on the nosepiece that touches the nostril rim to help ensure a seal. The acoustic pulse is then generated while the nosepiece is held still for 10 seconds. Sources of Variability Variation in the angle of incidence of the wave tube can cause a decrease in the depths of the I- and C- notches and a shifting of both anteriorly. Operator bias can have a significant effect on all parameters if tracings of suboptimal quality are accepted.
Giant aneurysms can occur rarely diabetes type 2 pathophysiology order actoplus met on line, with a vessel diameter greater than 8 mm, and these carry a grave risk for thrombosis, rupture or myocardial infarction. Children who develop coronary artery abnormalities will require long-term follow-up. Other common findings include extreme irritability, arthritis, diarrhea and vomiting, aseptic meningitis, hydrops of gallbladder and erythema and induration at Bacillus Calmette-Guérin scar. Thrombocytosis is evident after the first week of illness and may be an outstanding feature. Echocardiography will detect coronary artery involvement in the form of increased echogenicity, coronary ectasia, aneurysm formation and also evidence of carditis. This should be done preferably by a pediatric cardiologist on admission, again during subacute phase and at the end of 68 weeks. Other abnormalities like valvular leak, pericardial effusion and left ventricular dysfunction seen in the initial stages will usually subside without any sequelae. These should be administered as soon as diagnosis is made, positively within 10 days of onset vip. Aspirin is given in a dose of 80100 mg/kg daily in four divided doses during the acute phase and then continued in a smaller anti-thrombotic dose of 35 mg/ kg daily. At the end of 8 weeks aspirin is discontinued, if cardiac evaluation does not indicate any coronary artery involvement. Otherwise, aspirin should be continued until full regression of coronary arteries occurs, occasionally lifelong. Addition of clopidogrel or rarely warfarin should be considered for children with large multiple aneurysms. Selected patients with severe coronary artery stenosis may need coronary angioplasty, stenting or bypass surgery. Remainder may progress to stenosis, occlusion and myocardial infarction at a relatively young age. These children should be monitored periodically for risk factors for atherosclerosis like hypertension, hyperlipidemia and counseled on avoidance of smoking and obesity. Prognosis Kawasaki disease is usually a self-limiting disease, although without treatment about 25% children can develop serious coronary artery disease. With early recognition and adequate treatment, full recovery can be expected in majority of cases 918 vip. In view of the multisystem involvement, the clinical presentation can be very variable and one has to have a high index of suspicion. It has not been reported very frequently from our country but there is no reason to believe that it would be rare in India. According to the criteria given by the Centers for Disease Control and Prevention a definitive diagnosis of Lyme disease can be made when there is erythema migrans (> 5 cm diameter) or any one of the typical clinical features (arthritis, meningitis, radiculoneuritis, mononeuritis, carditis) in the presence of specific antibodies. It may be noted that all serological tests may be negative in the first few weeks of the illness and the treating physician may get virtually no help from the laboratory. Early disease can be treated with oral amoxicillin (50 mg/kg/day) while for disseminated disease or late cases parenteral ceftriaxone (100 mg/kg/day) is the drug of choice. Children treated late or incompletely can have a smouldering chronic course often resistant to any forms of therapy and resulting in considerable morbidity. The diagnosis can be made on the basis of criteria provided by Bohan and Peter: · Characteristic heliotrope discoloration over the upper eyelids · Symmetrical proximal muscle weakness · Elevated levels of muscle enzymes (aspartate aminotransferase, alanine aminotransferase, creatine kinase, aldolase) · Electromyographic evidence of myopathy · Muscle biopsy showing myonecrosis, myophagocytosis, and perifascicular atrophy. Treatment involves use of intravenous boluses of parenteral steroids (methylprednisolone 30 mg/kg/day or dexamethasone 5 mg/kg/day) for 35 days followed by oral prednisolone (1. Oral weekly methotrexate (1525 mg/m2/week) is now increasingly being used as first-line therapy in combination with prednisolone. Diffuse cutaneous systemic scleroderma is usually associated with widespread visceral involvement including the gastrointestinal tract, heart, lungs and kidneys. It is believed that fetomaternal graft-versus-host reactions are involved in the pathogenesis of this condition. Onset of disease is insidious and may be difficult to recognize in the initial stages. In addition, many children have abnormalities of nail fold capillaries which can be seen as capillary dropouts and dilated loops with a magnifying glass or the +40 lens of the ophthalmoscope. Onset of hypertension and proteinuria usually indicate renal involvement and should be a cause for serious concern. Penicillamine and colchicine can produce beneficial results in some patients, especially if used early in the course of disease. Monthly pulses of intravenous cyclophosphamide (followed by maintenance daily azathioprine or weekly methotrexate) can be life-saving in patients with interstitial lung disease. With appropriate management, 10-year survival rates of up to 90% have been reported in children. Scleredema is a benign, self-limiting condition characterized by non-pitting indurated edema over face, neck, shoulders and chest but always excluding the hands and feet. Treatment must be individualized and should focus on the particular disease component which is predominating in a given child. It is prepared by fractionation of pooled plasma obtained from remunerated healthy donors and consists of normal intact polyspecific IgG. These donors are subjected to strict screening procedures and the quality of the end product essentially depends on the quality of this screening.
Actoplus Met Dosage and Price
Actoplus Met 500mg
- 30 pills - $34.48
- 60 pills - $56.55
- 90 pills - $78.62
- 120 pills - $100.69
- 180 pills - $144.83
- 270 pills - $211.03
- 360 pills - $277.24
In lumbar segments metabolic disorder journal 500 mg actoplus met buy with mastercard, the anterior horn has a distinct medial extension, whereas in sacral segments, the anterior horn extends laterally. The posterior horn in both thoracic and cervical segments is narrow compared with lumbar and sacral segments. The thoracic segments have the least amount of gray matter, both anteriorly and posteriorly. Nevertheless, because the white matter contains axons transmitting information between the spinal cord Posterior median sulcus Laminae the spinal gray matter can also be divided into laminae or layers based on layerings of morphologically similar neurons. Acute spinal cord injury can result from trauma or stroke, while chronic injury can result from infections, inflammation, tumors, genetic disorders, and compression. A combination of trauma and vascular interruption comes with contusions to the spinal cord. While an actual transection of the spinal cord may not occur, contusive "bruising" of the spinal cord nonetheless results in a lesion that culminates in vascular insufficiency and necrosis (physiologic transection). A contusion injury is followed by the breakdown of the central core of the spinal cord, the formation of a cyst leading to the production of a hollow cavity, with inflammation and glial scar in surrounding intact tissue. The surrounding white matter, especially at the periphery of the damaged area, can survive and continue to transmit ascending and descending impulses. At what three intervertebral articulations are dislocations most likely to occur and what spinal cord segments are related to each What are the distinguishing characteristics of transverse spinal cord sections at sacral, lumbar, thoracic, and cervical levels Shorter individuals, compared to taller people, have less space between the end of the cord and the end of the vertebral canal. Damage to the brainstem is manifested by somatosensory or motor dysfunctions or both, accompanied by abnormalities in cranial nerve functions. The brainstem is the stalk-like part of the brain that is located in the posterior cranial fossa. The brainstem is covered posteriorly by the cerebellum to which it is connected by huge masses of nerve fibers that form the three pairs of cerebellar peduncles. Its anterior surface is closely related to the clivus, the downward sloping basal surface of the posterior cranial fossa between the dorsum sellae and foramen magnum. Clinical Connection A life-threatening event involving the brainstem can occur when a lumbar puncture is performed in a patient with increased intracranial pressure. Pressure on cardiovascular and respiratory centers in the medulla quickly results in death. Chapter 3 Brainstem: Topography and Functional Levels 29 of the medulla forms the caudal or medullary part of the floor of the fourth ventricle, the cerebrospinal fluidfilled cavity between the cerebellum and the pons and open medulla. Because these rootlets eventually join and are distributed with the vagus nerve, the so-called cranial part of the accessory nerve is considered by many to be a misnomer. Posteriorly, it forms the floor of the rostral part of the fourth ventricle, and it is covered by the cerebellum to which it is attached by the middle cerebellar peduncles or brachii pontis. An imaginary line passing from side to side through the cerebral aqueduct divides the midbrain into a posterior part or roof, the tectum, and an anterior part, the cerebral peduncle. The shallow basilar sulcus near the midline is normally occupied by the basilar artery. On the anterolateral surface of the pons about midway between the medulla and midbrain is the attachment of the trigeminal (V) nerve. This nerve consists of a larger inferolateral sensory root (portio major) and a small superomedial motor root (portio minor). Because only the most conspicuous anatomic landmarks Midbrain the anterior surface of the midbrain is formed by the cerebral peduncles. Posterior Surface Medulla the posterior surface of the closed or caudal half of the medulla contains the gracile tubercles on either side of the posterior median sulcus. The median sulcus divides the floor of the fourth ventricle into symmetric halves. Each half is further subdivided into medial and lateral parts by the superior and inferior foveae, small depressions at pontine and medullary levels, respectively. These foveae are remnants of the sulcus limitans and indicate the boundary between motor structures, which are medial, and sensory structures, which are lateral. Hence, extending laterally from the two foveae to the lateral recess is the vestibular area, and at the lateral recess is a small eminence, the acoustic tubercle. Its caudal part enlarges and is the facial colliculus, which overlies the abducens nucleus. Cerebellar Peduncles the cut surfaces of the cerebellar peduncles are at the lateral aspects of the pons and in the roof of the fourth ventricle. The massive middle cerebellar peduncle or brachium pontis is continuous with the basilar part of the pons. The superior cerebellar peduncle or brachium conjunctivum passes from the roof of the fourth ventricle into the tegmentum of the rostral pons. As a result, it receives input from all parts of the nervous system and, in turn, exerts widespread influences on virtually every central nervous system function, as described in Chapter 20. By locating on the brainstem specimen the same surface landmarks in a transverse section, one is able to determine precisely from where the section was taken. This is important because the clinician must project knowledge of the nervous system, no matter what the source, onto the gross brain and ultimately to the living brain in situ. Rostral Part of Closed Medulla the pyramids are anterior and separated by the anterior median fissure. The gracile and cuneate tubercles are posterior and separated by the posterior intermediate sulcus.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.