
Alli
General Information about Alli
Alli also presents a assist program that can help individuals stay on track and make the most out of the product. The program consists of personalised meal plans, exercise routines, and on-line assist from consultants. This added support can be useful for those who struggle to stay motivated during their weight loss journey.
It is crucial to notice that Alli isn't a magical capsule, and it does not work by itself. Individuals must comply with a low-calorie, low-fat food regimen and train often to see the best outcomes. Alli works hand in hand with a wholesome way of life to help individuals achieve their weight loss goals.
Alli is a weight loss help that works by blocking the absorption of fats within the body. It is the one over-the-counter weight reduction treatment that has been accredited by the FDA. Alli is a lipase inhibitor, which implies it prevents the breakdown of dietary fats, leading to fewer calories being absorbed by the physique.
Like any treatment, Alli may trigger some side effects. The commonest unwanted facet effects include oily stools, gasoline, and frequent bowel actions. However, these unwanted aspect effects are momentary and tend to enhance with time as the body adjusts to the medication. It is crucial to comply with the beneficial dosage and follow a low-fat diet to reduce the probabilities of experiencing these unwanted facet effects.
Weight loss is a battle that many people around the globe face. From strict diets to intense workout regimes, people typically strive varied strategies to shed those unwanted pounds. However, sometimes food regimen and train usually are not enough, and that's where Alli is obtainable in. Alli, also known as Orlistat, is an FDA permitted weight loss product that has been proven to help people lose about 50% more weight than with just dieting alone.
In conclusion, Alli is a trusted weight reduction product that has been confirmed to be efficient in combination with a wholesome life-style. However, it is essential to keep in mind that it isn't a magic capsule, and people must additionally put within the effort to see outcomes. If you are struggling to shed weight, give Alli a strive, however keep in mind to consult together with your doctor before starting any weight reduction medication or program.
There are many weight loss merchandise available on the market, however what differentiates Alli is its FDA approval. This signifies that the protection and effectiveness of the product have been examined and confirmed by the Food and Drug Administration. Alli can also be the primary over-the-counter weight reduction medication to be permitted by the FDA, giving it a strong reputation.
Alli works by targeting the enzymes that break down fats in the intestines. When taking Alli, these enzymes are blocked, and the fats is passed by way of the physique undigested. This process helps in lowering the number of calories absorbed by the body, leading to weight loss.
Another benefit of Alli is its availability. Unlike other weight reduction medicines that require a prescription, Alli may be bought over the counter at any pharmacy or online. This makes it easily accessible for people who could not have entry to a doctor or a prescription.
It is also clear that aminoglycosides have measurable vestibulotoxic and ototoxic effects weight loss dr oz discount 60 mg alli with amex. Fluroquinolones do not pose these threats and will treat both Pseudomonas aeruginosa and Staphylococcus aureus. Metronidazole gel can be useful if there is an otitis externa where anaerobes have been cultured. Tri-Adcortyl ointment (a substitute is now made by Mandeville Medicines in the United Kingdom) contains steroid, neomycin and gramicidin and also an antifungal medication. After thorough microsuction, this ointment can be instilled into the ear canal and left until the next appointment. There has been one reported case of ototoxicity in use with a perforated tympanic membrane. Topical steroid drops alone may be useful for patients that have inflammation secondary solely to allergy or sensitization rather than infection. An external ear canal wick, such as the Pope otowick (Xomed), expands into the canal, improving delivery of topical medicines. Glycerine and ichthammol impregnated ribbon gauze has a hygroscopic effect to reduce canal oedema and good antibacterial effect against Staphylococcus aureus and Streptococcus pyogenes, but not Pseudomonas aeruginosa. Topical aluminium acetate drops are as effective as antibiotic drops but are expensive, difficult to obtain and need to be freshly prepared. Systemic antibiotics are unnecessary unless there is extension outside the ear canal, immunosuppression, or local factors that hinder the delivery of topical preparations. Topical antifungal drops such as clotrimazole solution should be combined with regular aural toilette. Chronic otitis externa can be frustrating for both the patient and the doctor treating it. This consists of a polyvinylic acid film formed by a combination of a specific antibiotic and steroid drop along with acetic acid. The benefit may be due to the removal of the bacterial biofilm, giving longer-term results. An alternative strategy in antibiotic-resistant chronic otitis externa may be a single dose of therapeutic bacteriophage preparations. These are viruses that can break down the biofilm to specifically destroy bacteria and then self-replicate until that bacteria is no longer present. Choice of topical antibiotic drop shows little difference in resolution of symptoms, except in the case of microbial resistance, and with the increased recognition of Pseudomonas aeruginosa, infection the topical use of quinolones is likely to be important. Remember potential allergens and the possibility of fungal infection in those ears that have already had prolonged treatment. Effective delivery of medication is important; therefore, microsuction and the use of an ear wick can be beneficial. Fresh water swimming as a risk factor for otitis externa: A case control study Archives of Environmental Health. Cholesteatoma is the most common tumour found in the middle ear but will not be discussed further given the detailed description given elsewhere in this textbook. Glomous jugulare arises from the jugular bulb and tends to be larger, involving the jugular foramen and adjacent structures. Glomus tumours are more common in females and tend to present in adults over the age of 40. Myringosclerosis of the tympanic membrane can make visualization of a lesion difficult, and imaging is often vital to ensure a correct diagnosis and treatment plan is made. Hearing 514 Tumours of the middle ear location and size, the most widely used being that of Fisch and Oldring. It is important to obtain imaging of the lesion to differentiate a glomus tumour from 1. If required, feeding vessels may be embolized radiologically shortly before any planned surgery. This must be evaluated preoperatively to avoid catastrophic hypertensive changes that can ensue when removing the tumour. In other cases, however, the lesion may arise from the promontory, in which case a rounded red lesion is seen. In more advanced cases the lesion may have extruded into the ear canal, producing a friable polyp prone to bleeding. In many patients, watchful waiting is sufficient as smaller tumours may not grow and reassurance once a diagnosis has been established is sometimes enough. If this route is followed it is important to properly stage the tumour and monitor progress indefinitely. Excision of a glomus tympanicum can be a bloody affair unless preoperative planning is adequate. Resection of a glomus tympanicum can usually be performed by an endaural route, sometimes with only a permeatal incision. It may be necessary to stage the tumour resection in some cases if excessive Benign middle ear tumours / Adenomas 515 bleeding occurs as visualization of the fallopian canal is important to avoid laser damage to the facial nerve. Glomus jugulare Although these tumours are derived from the same tissue as tympanicum tumours neural crest cells they are more difficult to treat owing to their association with the jugular bulb. Larger tumours may present with cranial nerve involvement, with facial nerve and vagus nerve palsies being the most common associated neuropathies. The highly invasive nature of these tumours, together with their insidious and slow growth along paths of least resistance, means that resection tends to occur late and can be associated with significant morbidity.
The presentation for viral labyrinthitis is as for a vestibular neuronitis weight loss pills dexatrim alli 60 mg purchase, with the addition of hearing loss that is permanent. Specific causes include mumps and herpes zoster reactivation (Ramsay Hunt syndrome). Lyme disease can lead to vertigo with a sensorineural hearing loss as a consequence of infection by the spirochete Borrelia carried by deer ticks. A history of travel to an endemic area with perhaps an erythematous rash at the site of a tick bite indicates the need to test for specific antibodies. Treatment with antibiotics is effective and prevents chronic neurological sequelae. Management is expectant unless a perilymph fistula is present and symptoms of vertigo persist. Iatrogenic trauma needs to be considered after middle ear surgery and especially after cochlear implantation when vertigo is a reasonably common sequel. Prevention is important, but if damage has occurred, surgery is indicated in the case of perilymph fistula and hyperbaric oxygen in the case of decompression sickness. Perilymph fistulae can present with fluctuating vertigo and progressive hearing loss associated with straining and stooping or other actions that change pressure across the fistula. Whether spontaneous perilymph fistulae arise in anatomically normal ears is a subject of debate, but the general consensus is that they do not. The pathology is considered to be caused by shifting of loose otoconia into a semicircular canal, usually the posterior, with stimulation of the cupula and resultant short-lived vertigo on postural change, particularly lying on one side. The DixHallpike positioning test will provoke both symptoms and rotatory nystagmus towards the downmost ear. The nystagmus is delayed in appearance, resolves after about 40 seconds and is reversed on sitting up again. Repetition of the manoeuvre leads to a reduction in severity of both the symptoms and the nystagmus. The presentation is usually of a progressive hearing loss with vestibular disturbance. Additionally, there are usually other symptoms or signs of autoimmune disease, such as eye inflammation. Treatment is with steroids and other immunosuppressants, and management should be joint with a paediatrician. The only cases seen by the author are those with a strong family history, raising the question of a genetic mutation. Symptoms are of episodic vertigo with tinnitus and a feeling of pressure in the ear with a fluctuating low-frequency sensorineural hearing loss. Management is with a low-salt diet and the use of thiazide diuretics as in adults, with more radical treatments used with considerable caution. Dehiscent superior semicircular canals are a recognized cause of Tullio phenomenon (vertigo induced by noise) in adults but are rarely seen in children. As with most dominantly inherited conditions, de novo mutations occur reasonably frequently (~50 per cent). Vestibular function is compromised, but the onset is gradual and with unilateral tumours, symptoms of vertigo and imbalance are rare. Migraine and migraine equivalents Migrainous pathology is the most common cause of episodic vertigo in children and can present at any age. The vertigo is episodic and usually short lived, particularly in younger children, there are no interictal phenomena of note and there is a family history in 50 per cent or more of cases. The presentation is dependent on age and headache is a rare accompaniment in the younger child, although may become more of a problem in the second decade. Investigation can reveal subtle signs of central vestibular dysfunction, but generally most measures of audiological or vestibular function are within the normal range for the age of the child. Aminoglycosides are ototoxic, and some, such as streptomycin and gentamicin, are highly vestibulotoxic. The use of aminoglycosides in sick neonates is common and the effect on the vestibular system largely unknown. Monitoring the levels of aminoglycosides during treatment and avoiding high serum levels is useful in prevention of both hearing loss and vestibular damage. Cisplatin is a chemotherapeutic agent used widely in the treatment of sarcomas, lymphomas and germ cell tumours. It is known to give rise to a dosedependent high-frequency hearing loss, and there Causes of balance disorder / Epilepsy 631 Table 66. Migrainous vertigo, a common cause of episodic vertigo in children, accounts for a third or more cases of vertigo presenting to a balance clinic. The vertiginous episodes occur in clusters and can be predictable in their periodicity. They can last from a few minutes to several hours and are usually accompanied by other migrainous phenomena such as visual or olfactory aura, photophobia, phonophobia and prostration. These episodes are not usually accompanied by headache (acephalgic) in children, although when they are it can help with the diagnosis. Presenting in the first year of life, it includes episodes of torticollis usually accompanied by distress, pallor and instability with occasionally vomiting. The episode lasts a few minutes, during which the child is pale and unwell, and the cessation of the episode is sudden and complete. Sometimes these episodes are Also related are abdominal migraine, which can present with abdominal pain and vomiting, and cyclical vomiting. Common precipitants include caffeine, chocolate, cheese, citrus fruits and monosodium glutamate, and keeping a diary often identifies these.
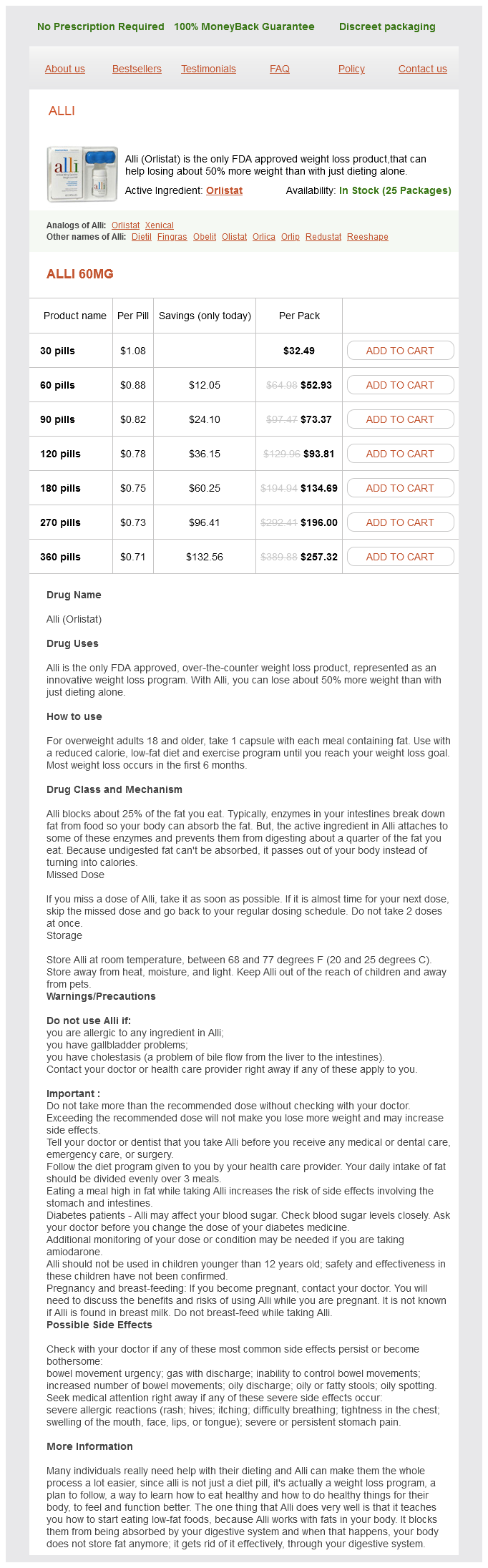
Alli Dosage and Price
Alli 60mg
- 30 pills - $32.49
- 60 pills - $52.93
- 90 pills - $73.37
- 120 pills - $93.81
- 180 pills - $134.69
- 270 pills - $196.00
- 360 pills - $257.32
The inclusion of specialized personnel in the initial communication process may support rendering institutions appropriate treatment strategies while decreasing diagnostic discordance weight loss drops buy alli with mastercard. This access should be staffed 24 hours per day, 7 days per week and should be unencumbered. The ability to support communication among the referring physician, the dispatcher, and the medical control officer simultaneously can speed up decision making and the initiation of transport. Changes in weather, patient status, equipment needs, and bed status need to be communicated in a timely manner. This information may demand a review of the transport plan and is best facilitated through a central communication center. This medium permits the use of satellite technology and video-conferencing equipment to conduct a real-time consultation between medical specialists in two geographically different areas. These technologies may facilitate appropriate referral of patients according to complexity and may decrease incidence of inappropriate transfer or diagnostic discordance, allowing for optimal use of resources. Quality the regional subspecialty perinatal care center, as noted in Table 3-1, is responsible for regional outreach support, education, and continuous quality oversight. However, in light of current health care complexities and regulatory specifications surrounding the quality and safety of patient care, it is recommended that this role be assigned to an individual with the expertise to effectively evaluate programmatic performance at all levels of the organizational structure. This continuous evaluation of the process will facilitate modification of the transport system when potential problems are identified. The systematic collection and analysis of carefully selected performance indicators such as patient demographics, management and outcome data, safety standards, logistics, equipment malfunction, and cost will drive quality initiatives. A quality review of individual transports, incidence reports, and occurrence debriefs will enhance this process. Transport programs must create individualized internal training programs that effectively provide current and continuous education to ensure maintenance of appropriate skills for highquality perinatal transport. A similar program must be adapted to provide educational resources to the referring hospital where training in pretransport resuscitation and stabilization is imperative. Ensuring competence in these areas has the potential to improve short-term and long-term morbidity of sick infants, offsetting the negative effects of deregionalization and distance between interhospital transfer facilities. Adequate re erral o high-risk perinatal patients begins with high-quality antepartum surveillance. Early identification of factors that can affect pregnancy outcome is important in developing appropriate diagnostic and treatment plans. Optimal perinatal care implies having well-trained and up-todate obstetricians at all levels of care during both the antepartum and intrapartum period. These physicians should be experts in identifying maternal-fetal risk factors and complications through their knowledge, clinical skills, and expertise in prenatal ultrasound and fetal monitoring. Consultation and referral decisions for the high-risk mother should be based on the results of a thorough evaluation of each patient and specific guidelines. Communication between the referral center and the regional perinatal center may be facilitated through the use of video-medicine technology. Beyond the immediate delivery room setting, supportive care should be offered and maintained until the transport team has arrived and assumed care (Box 3-2). L: stabilization care of sick infants-guidelines for neonatal healthcare providers, ed 6, Park C U 2013, S. Prevention of adverse events and delivery of safe patient care are stressed throughout the program. Although the reasons for neonatal referral may be quite diverse and based on needs of infants relative to the capabilities of the referring center, the most common indication is respiratory distress of the neonate. The importance of this form of continuing dialogue with respect to accuracy in diagnosis, management, and changes in patient status cannot be stressed enough. Again, the use of video-telemedicine may facilitate the accuracy of these interactions. Many health care pro essionals can have medical responsibility or a single patient at one time. The fact that one person has acquired medical responsibility does not automatically release someone else. O n arrival of the transport team, collaborative management is of upmost importance. While the patient remains in the referring facility the referring physician cannot hand off the patient and proceed as if the patient has left the facility and his or her care. The referring facility allows the specialty team to provide care under the supervision and authority of the referring physician. The referring physician retains involvement and ultimate responsibility and signs the transfer certificate at the time of actual transfer. A team approach is in the best interest o the patient and should involve all participants in the process. Communication between the referring physician, the transport team, and the accepting physician is of great importance. O n leaving the referring facility, the transport team and receiving facility assume responsibility and control for medical decision making. Provision of intensive care in the transport environment incorporates the philosophies of neonatal and pediatric critical care, but in a mobile environment with physical and environmental constraints of staff, space, mobility, and equipment. It is important to recognize that the physical requirements o team members are di erent rom those who work solely in a hospital or clinic environment. Team members will be required to lift patients or carry equipment often with little or no help. Personnel should not be unusually prone to motion sickness or have mastered the techniques to mitigate the effects of motion sickness. In the event that a team member is unable to function, patient and crew safety may be compromised because there are few options should a team member be incapacitated while on duty. For this reason team members with certain medical conditions may be at least temporarily precluded from participation on a transport.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.