
Arzomicin
General Information about Arzomicin
Arzomicin comes in numerous types, together with tablets, oral suspension, and intravenous solution. The dosage and length of treatment rely upon the kind and severity of the an infection, as properly as the affected person's age and medical history. It is important to observe the prescribed dosage and finish the whole course of therapy to ensure complete eradication of the infection and forestall the development of antibiotic resistance.
Arzomicin, also recognized by its brand name Zithromax, is a robust macrolide antibiotic used to deal with a variety of bacterial infections. This medicine belongs to the identical class of antibiotics as erythromycin and clarithromycin, but its unique chemical construction permits for an extended duration of motion and a more effective therapy in opposition to a variety of micro organism.
Ear infections, also recognized as otitis media, are a standard childhood sickness that may additionally affect adults. They occur when the middle ear becomes infected and inflamed, causing symptoms corresponding to ear ache, fever, and issue hearing. Arzomicin is an effective remedy for ear infections attributable to sure micro organism, similar to Haemophilus influenzae, Streptococcus pneumoniae, and Moraxella catarrhalis.
Like all antibiotics, Arzomicin might trigger some side effects, though not everyone will expertise them. The most common side effects embrace nausea, vomiting, diarrhea, and stomach pain. In rare circumstances, it could possibly cause extra extreme side effects similar to liver problems, allergic reactions, and listening to loss. It is necessary to tell your doctor should you expertise any concerning unwanted facet effects whereas taking Arzomicin.
Certain precautions ought to be taken when utilizing Arzomicin. It isn't beneficial for sufferers with a recognized allergy to macrolide antibiotics or those who have liver or kidney illness. It may interact with other drugs, so it could be very important inform your physician of some other medicines you're taking.
One of the most typical infections Arzomicin is prescribed for is respiratory tract infections, such as ear infections and pneumonia. It works by inhibiting the growth of micro organism and stopping their capability to reproduce, ultimately clearing the an infection and relieving signs.
In conclusion, Arzomicin (Zithromax) is a highly efficient macrolide antibiotic used to deal with a variety of bacterial infections, particularly these of the respiratory tract. It is extensively prescribed due to its broad spectrum of exercise and minimal unwanted aspect effects. However, you will need to take this medicine as prescribed and notify your doctor of any regarding side effects. With proper use, Arzomicin can successfully treat infections and improve general health and well-being.
Aside from respiratory infections, Arzomicin can be used to treat other bacterial infections such as pores and skin and gentle tissue infections, sexually transmitted illnesses, and sure types of gastrointestinal infections.
Pneumonia, on the opposite hand, is a more severe an infection of the lungs that could be brought on by numerous micro organism, viruses, and fungi. It can vary from gentle to severe and even life-threatening if left untreated. Arzomicin is often prescribed as a first-line therapy for community-acquired pneumonia due to its effectiveness against Streptococcus pneumoniae, Haemophilus influenzae, and Mycoplasma pneumoniae.
In other tumor types antibiotics history arzomicin 250 mg purchase without prescription, especially melanoma, there appears to be no such correlation. This is difficult to do via an endoscopic approach, and patients are usually required to have a more invasive radiological biopsy that requires greater expertise and carries an increased risk of complications such as bleeding and pneumothorax. Levels of immune proteins in peripheral venous blood samples are currently being evaluated as potential biomarkers of response. Preliminary data suggest that elevated systemic inflammatory markers may identify patients who are less likely to benefit from 77 © 2017 Health Press Ltd. Further clarification of this relationship, and determination of the optimal systemic inflammatory marker, may improve patient selection and provide options for future combination therapies. Such analyses are likely to be less useful in earlier stages of disease when inflammatory markers are less frequently elevated. However, to date, patients with lung cancer have not tolerated the same doses as those given to patients with melanoma. Studies are under way with combinations of established immunotherapies and new agents that target other immune regulatory molecules, including activating antibodies that target agonistic immune receptors and inhibitory antibodies that target inhibitory immune receptors. It is hoped that these combinations will be efficacious in malignancies that are currently resistant to immunotherapies. Clearly, the optimal use of vaccines and other immunotherapies in combination with standard systemic therapies, radiotherapy and surgery needs to be established. Early data from patients with lung cancer suggest that added benefit can be obtained from the combination of chemotherapy and immunotherapy. Multiple trials are under way to determine whether there is benefit in adding an immunotherapeutic agent be it a checkpoint inhibitor, or a vaccine or their combination to chemotherapy, targeted agents or other systemically delivered anti-cancer therapies. It will be exciting to see if concurrent or prior use of other systemic therapies might increase mutational burden, and thereby improve the response to immunotherapies. Radiotherapy is widely used to treat patients with malignancy in a number of settings, including curative, adjuvant and palliative treatment. As well as external beam radiotherapy and brachytherapy, radiation is also involved in the form of therapeutic isotopes and selective internal radiation delivery. Clinical trials are under way to determine the optimal dose and scheduling of radiotherapy to combine with immunotherapies. It appears that standard scheduling of radiotherapy provides more favorable immune interaction than hypofractionated schedules. The future of immuno-oncology will be to define whether these agents might be more effective when given in the postoperative adjuvant setting, or even in the neoadjuvant setting prior to definitive surgery. In preclinical murine models of triplenegative breast cancer, neoadjuvant immunotherapy involving depletion of regulatory T cells reduced rates of metastatic disease and increased numbers of long-term survivors compared with the same treatment given in a postsurgical adjuvant fashion. A number of studies of neoadjuvant therapy in various tumor settings are under way. The duration of therapy in clinical trials is highly arbitrary: for example, the duration of ipilimumab treatment in patients with melanoma was 4 doses over 3 months in the metastatic setting, and up to 3 years in the adjuvant setting. It is currently unclear whether long-term responders need ongoing costly infusions of these immunotherapies at the same dosing intervals. Overall toxicities are less than with chemotherapy, but a small percentage of patients experience severe and lifethreatening toxicities such as colitis, pneumonitis, hepatitis and neurological impairment, including GuillainBarre syndrome. An ability to predict or completely control toxicities would greatly enhance the use of combination immunotherapies. Similarly, it would be helpful to know how to use these agents safely in patients with pre-existing autoimmune diseases, transplant recipients and those with intercurrent infection. Precision immunotherapy Immuno-oncology has made incredible advances in recent years. In order to harness the immune system for enhanced anti-tumor response and deliver optimal immunotherapy to every patient, predictive biomarkers and novel combination treatment strategies are urgently needed. In the future, the one size fits all model will become obsolete, and precision immunotherapy will be tailored to each individual to radically improve their outcomes. Key points the future of immuno-oncology · Predictive biomarkers are urgently needed to direct precision immunotherapy. Immuno-oncology: allying forces of radio- and immunotherapy to enhance cancer cell killing. Improved efficacy of neoadjuvant compared to adjuvant immunotherapy to eradicate metastatic disease. Some chronic diseases are major killers and are responsible for roughly 70% of all deaths and for 86% of our health care dollar. The Chronic Care Model addresses the rising health care demands of chronic diseases. The goal of this model is to improve the quality and cost-effectiveness of care for patients. In addition, this chapter describes the different types of palliative care and the need to make a quality end-of-life plan before a medical crisis arises. T Defining Chronic Diseases In the 21st century, we can expect to live longer than any previous generation. However, there are more than 133 million people-almost one out of every two adults-living with at least one chronic disease (Anderson, 2007, 2010). For many, having a chronic disease means living with an illness for years if not a lifetime. As defined in Chapter 2, a chronic disease or chronic condition begins slowly and lasts anywhere from more than 3 months to a year or more. Chronic diseases generally are not immediately fatal, but they are also rarely completely cured. Some people use the term chronic condition instead of chronic disease because there is social stigma associated with having a "disease. Regardless of which term is used, having a chronic disease is a health condition that requires ongoing care, limits what the person does, and can last a lifetime.
Therefore the onset of inflammation can affect the regulation of many target genes including drugmetabolizing enzymes virus like ebola discount arzomicin 250 mg with amex, membrane transporters, and their transcription factors. Changes that occur during an acute inflammatory response are generally transient, lasting only a few days once the inflammatory response is resolved. Most frequently, rodent models of acute inflammation are employed due to practical and ethical concerns, and they have been well characterized in the past. Physiological changes similar to humans can be achieved in these models by administration of bacterial, viral, protozoal, or chemical agents or by direct exposure to proinflammatory cytokines. It is used to model bacterial infections or sepsis and is known to result in a highly reproducible induction of proinflammatory cytokines, as well as physical symptoms such as fever and hypotension (Copeland et al. The subcutaneous administration of turpentine, an organic solvent distilled from pine resin, is also frequently used to model aseptic acute inflammation or trauma in rodents. The subcutaneous injection of other irritants such as carrageenan or magnesium silicate (talc) has also been used to model acute inflammation. As inflammation-mediated changes in gene expression are thought to be attributed through cytokine-mediated pathways, cytokines can often be directly administered in vitro, and in vivo, to initiate the inflammatory response. Indeed, cytokine levels are frequently measured to monitor the inflammatory response to bacterial and viral mimetics. Although it is difficult to directly translate rodent models to the clinical setting due to species differences in drug disposition and gene isoforms, it has been shown that there are similarities in the release of cytokines, activation of transcriptional factors, and gene expression changes in humans and rodents during an acute inflammatory response (Copeland et al. However, emerging evidence in the last two decades has revealed the association of altered drug transporter expression due to an inflammatory response. As many therapeutic agents are transferred across epithelial membranes via transporter proteins, they play a pivotal role in altered pharmacokinetics during inflammation. Subsequent studies also expanded to examine inflammatory-mediated changes in other epithelial membrane barriers. Although the acute inflammatory response is known to alter the expression of many liverderived proteins, the effect of inflammation is not limited to the liver, and changes can be seen in epithelial tissues of the intestine, kidney, brain, and placenta. These transporters are ubiquitously expressed in the apical or basolateral membranes of numerous organs such as the liver, kidney, intestine, brain, heart, lungs, placenta, uterus, mammary gland, and testis among others. Within this group of transporters, a few are of particular importance, as they are also known to transport clinically important drugs. It is thought to play a protective role by secreting potentially toxic endogenous and exogenous compounds across epithelial membranes, thereby preventing drug entry or 64 3. Specifically, it is located at the endothelium of the bloodebrain barrier and testis, on the apical surface of hepatocytes, intestinal enterocytes, proximal renal tubules, and placental syncytiotrophoblasts. It transports a broad range of chemically diverse substrates, including many chemotherapeutic agents. Indeed, overexpression of P-gp at the cell surface of tumors is an important contributor to multidrug resistance. One of the first in vivo reports demonstrated an inflammation-mediated downregulation of P-gp in both the turpentine and endotoxin models of acute inflammation. As compared with controls, a significant 70e80% decrease in the hepatic protein expression of P-gp was seen in turpentine- or endotoxin-treated male rats. Furthermore, P-gp-mediated efflux of rhodamine 123 (a known P-gp substrate) was decreased by 45e60% in hepatocytes isolated from these rats (Belliard et al. As there are two isoforms that encode for P-gp in rodents, differences in their regulation have been observed in several instances. On the other hand, hepatic protein expression is downregulated in both species (Sukhai et al. These findings are in line with pharmacokinetic studies that have demonstrated that changes in transporter expression leads to functional changes of the protein. Studies in mice have shown that the endotoxin-mediated downregulation of Abcb1a in liver is associated with a 50% decrease in biliary clearance of the P-gp substrate doxorubicin as well as reduced systemic clearance of the drug (Hartmann et al. Likewise, the endotoxin-mediated downregulation of Abcb1a in rat liver is associated with corresponding increases in the hepatic accumulation of 99m Tc-sestamibi and decreased biliary secretion of digoxin, both of which are substrates of P-gp (Wang et al. Efflux transporters such as P-gp, which are highly expressed in the intestinal epithelium, play a role in limiting absorption of many clinically important compounds. As such, it is critical to understand the alterations that are imposed during inflammation. An inflammation-mediated decrease in the jejunal and ileal expression of Abcb1a along with a corresponding decline in the basolateral to apical efflux of the P-gp substrates, amiodarone and rhodamine 123, has been reported in endotoxin-treated rats (Kalitsky-Szirtes et al. Increased plasma concentrations of tacrolimus in transplant patients suffering from infectious diarrhea (Berengue et al. The discrepancy between results is not clear at present; however, different methods, cytokines, or cell lines may play a role. The discrepancy between results is not clear at present; however, different methods, species, and models of inflammation may play a role. These changes, however, did not affect the functionality of the protein, as the uptake of the P-gp substrate rhodamine 123 was unaffected (Poller et al. The transient change in protein expression was not found to alter the transport of doxorubicin across the bloodebrain barrier. These transporters are believed to play a protective role by preventing entry or facilitating efflux of potentially harmful endogenous and exogenous substrates from the fetal compartment. Preclinical studies conducted in pregnant rats treated with endotoxin and poly I:C have demonstrated induction of proinflammatory cytokines along with time- and dose-dependent decreases in Abcb1a and Abcb1b placental gene expression (Petrovic and Piquette-Miller, 2010; Wang et al. Changes in P-gp expression were also associated with an increased accumulation of the substrates digoxin, Tc-sestamibi, and lopinavir in the fetal compartment of pregnant rodents, suggesting comprised function of this transporter under inflammatory stress (Petrovic and Piquette-Miller, 2010; Wang et al. Interestingly, observed changes in fetal livers were similar to those seen in maternal liver. However, due to the nature of human studies, neither was sufficiently powered to detect changes in protein expression or at term, and thus additional studies are needed. Originally discovered in a breast cancer cell line exhibiting multidrug resistance to chemotherapeutic agents, it is now known to transport a wide array of drugs as well as endogenous compounds (Ni et al.
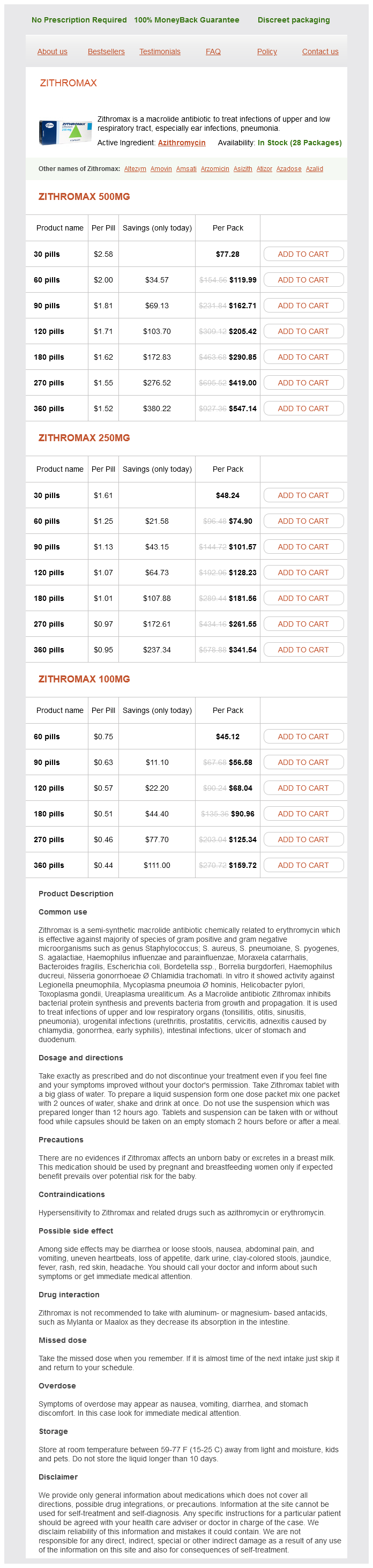
Arzomicin Dosage and Price
Zithromax 500mg
- 30 pills - $77.28
- 60 pills - $119.99
- 90 pills - $162.71
- 120 pills - $205.42
- 180 pills - $290.85
- 270 pills - $419.00
- 360 pills - $547.14
Zithromax 250mg
- 30 pills - $48.24
- 60 pills - $74.90
- 90 pills - $101.57
- 120 pills - $128.23
- 180 pills - $181.56
- 270 pills - $261.55
- 360 pills - $341.54
Zithromax 100mg
- 60 pills - $45.12
- 90 pills - $56.58
- 120 pills - $68.04
- 180 pills - $90.96
- 270 pills - $125.34
- 360 pills - $159.72
Women who have babies after age 30 or are taking fertility drugs have an increased chance of giving birth to more than one baby bacteria yersinia enterocolitica arzomicin 100 mg generic. Pregnancy with multiples can cause premature births and low birth weights as well as carry higher risk of disabilities. This condition causes high blood pressure, and protein buildup in the urine of pregnant women. Preeclampsia can result in kidney failure, seizures, and death, as well as early delivery. Labor that begins before 37 weeks of pregnancy puts both the mother and baby at increased risk for health problems. Signs of miscarriage include vaginal bleeding, cramping, or fluid and tissue passing from the vagina. During these visits, the woman is examined, and the growth of the baby is checked. Even before considering becoming pregnant, a woman should see a health care provider for preconception care. Pregnancy and Delivery A normal pregnancy is approximately 40 weeks, and it is divided into three trimesters. In the first trimester (weeks 112), the sperm fertilizes the ovum, causing cells to form the fetus and the placenta. In the second trimester (weeks 1328), a woman can find out the sex of her infant. Muscle tissue, bone, and skin have formed; movement begins; and the fetus sleeps and wakes regularly. The survival rate for babies born at 28 weeks is about 92%, although those born at this time can have serious health problems. By the third trimester (weeks 2940), bones are soft and yet almost fully formed, and the eyes open and close. Infants born before 37 weeks are preterm and are at increased risk for health problems. At 37 weeks, the fetus is full term and can usually survive without support if delivered. However, unless there is a medical issue, it is best to wait until at least 39 weeks to deliver. Labor is a three-stage process that results in the birth of the baby and the expulsion of the placenta. The third stage begins with the birth and ends with the completed delivery of the placenta. Just as pregnancy is different for every woman, the signs of labor and the length of time for each stage are different from woman to woman. Sometimes a woman may have an induced labor, in which medications are used to bring on labor if the health of the mother or the fetus is at risk. This surgery is necessary if a woman is carrying more than one fetus or if the labor is not going well. A breech birth means that the baby is upside down and that the feet are delivered first. Women who have a C-section are given pain medication-an epidural block, a spinal block, or general anesthesia. An epidural block is an injection in the spine that numbs the lower part of the body. A spinal block also numbs the lower part of the body by an injection directly into the spinal fluid. C-section delivery is safe, but it can increase the risk of having difficulties with future pregnancies. It is done either directly from the breast or by expressing, which is pumping out breast milk and bottle-feeding it to the baby. Breastfeeding is the recommended method for feeding babies because the milk has the right balance of nutrients to help a baby grow. Some nutrients in breast milk help protect babies against common childhood illnesses and infections. Certain medications, illegal drugs, and alcohol can also be passed through the breast milk to the baby. Diseases of the Female Reproductive System For purposes of discussion in this chapter, common female reproductive system diseases are split into three groups: diseases that cause abnormal uterine bleeding, diseases that cause inflammation, and cancers. Diseases That Cause Abnormal Uterine Bleeding Endometriosis is a disease in which uterine tissue grows somewhere else-for example, in the ovaries. Although many women have cramping during their menstrual period, women with endometriosis have severe menstrual pain that increases over time. Some women have no symptoms at all, and for them, having trouble getting pregnant may be their first sign. The cause of endometriosis is unknown, and it cannot be prevented, but there are risk factors for developing the condition, including the following: · · · · A family history of endometriosis Menarche at a young age Frequent periods or periods that last 7 or more days Never having had children Endometriosis is usually diagnosed in women in their 30s and 40s and is determined by signs and symptoms, pelvic exam, ultrasound, and laparoscopy. Treatment depends on severity and on whether the patient hopes to become pregnant. Regardless of the treatment, endometriosis is chronic, but signs and symptoms can improve after menopause.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.