
Aspirin
General Information about Aspirin
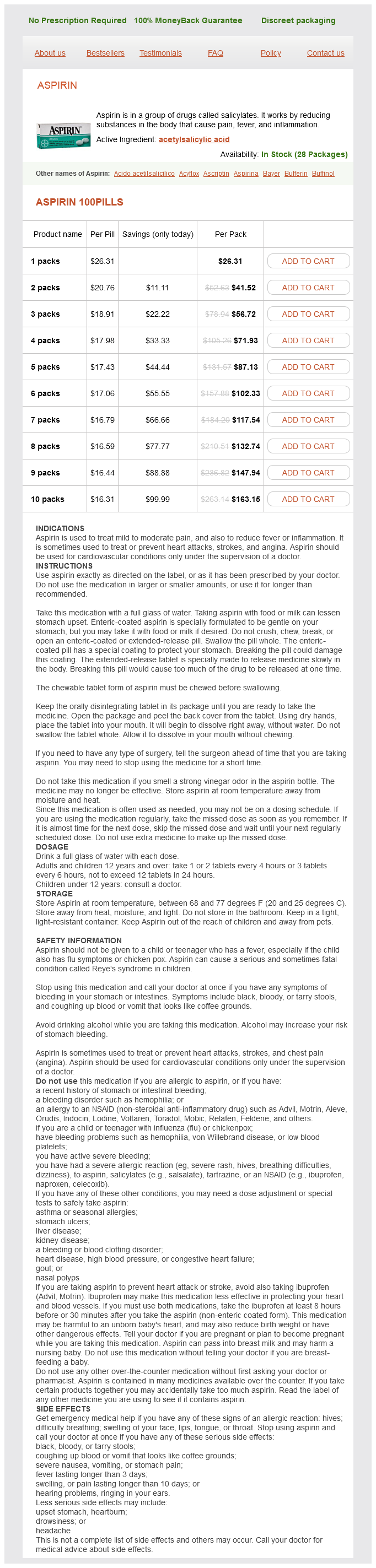
Aspirin, also referred to as acetylsalicylic acid, is a commonly used medicine for ache relief and fever reduction. It belongs to a gaggle of drugs called salicylates and is probably certainly one of the most generally used non-steroidal anti-inflammatory medication (NSAIDs). It is available over-the-counter, making it easily accessible to most of the people.
In conclusion, aspirin's effectiveness in relieving pain and reducing irritation has made it a extensively used and trusted treatment. Its antiplatelet effects and potential for preventing sure kinds of cancer have only added to its popularity. However, like several treatment, it should only be taken as directed and under the guidance of a healthcare skilled to avoid any potential unwanted effects. With correct use, aspirin could be a valuable tool in managing ache and improving overall well being and well-being.
One of the main causes for the widespread use of aspirin is its capability to alleviate ache and scale back irritation. Aspirin works by inhibiting the manufacturing of prostaglandins, which are chemical messengers that trigger ache and irritation in the physique. By blocking the production of these chemical substances, aspirin helps to cut back pain, swelling, and fever.
Despite its many advantages, like several medication, aspirin comes with its own set of potential unwanted effects. The most common aspect effect of aspirin is stomach irritation, which may range from mild discomfort to more severe circumstances such as ulcers and bleeding. To minimize these dangers, it is important to observe the beneficial dosage and never exceed the daily restrict.
Another potential aspect impact of long-term aspirin use is Reye's syndrome, a rare however critical situation that primarily impacts kids and young adults. This situation could cause severe liver and mind harm and can be deadly. As a precautionary measure, aspirin just isn't beneficial for individuals underneath the age of 18, until particularly prescribed by a physician.
In latest years, aspirin has additionally gained consideration for its potential position in preventing certain kinds of most cancers. Studies have shown that common aspirin use may scale back the danger of creating colorectal most cancers, and ongoing research is being performed on its potential benefits in stopping different types of cancer as properly.
Aspirin can be generally used to alleviate signs of varied situations corresponding to complications, colds, flu, and arthritis. It is also utilized in combination with other medicines to treat extra extreme ache, similar to migraines or menstrual cramps. Its versatility and effectiveness make it a popular selection for many people looking for aid from different sorts of discomfort.
The discovery of aspirin could be traced again to ancient times when people used willow bark to deal with pain and irritation. However, it was not until the nineteenth century that a German chemist, Felix Hoffmann, first synthesized aspirin in its pure type. Since then, it has turn into a household name and a staple treatment in every drugs cupboard.
In addition to its pain-relieving properties, aspirin additionally has antiplatelet effects. This signifies that it helps to forestall blood clots from forming by inhibiting the exercise of platelets, that are small cells discovered within the blood. This is why low-dose aspirin is usually prescribed to individuals with a excessive risk of heart assault or stroke.
However shoulder pain treatment yahoo discount aspirin 100 pills online, children with celiac disease have lower levels of circulating IgA antiepidermal Tgase when compared to adults with celiac disease, whereas levels of circulating IgA antibodies against tissue Tgase are not significantly different between children and adults with celiac disease. Whether the IgA skin deposits play a role in the pathophysiology of blister formation is not known. The finding of IgA and complement in almost all skin sites, not only in lesional skin, makes one postulate that if IgA (either alone or as a part of an immune complex) does play a role, additional factors are still needed to explain the initiation of lesions. It may be that after the initial neutrophilic infiltrate binds to the cutaneous IgA, factors such as cytokines, chemokines, and proteases are released that both directly result in blister formation and induce basal keratinocytes to produce collagenases or stromelysin-1 that further contributes to the formation of blisters. The availability of immunopathologic techniques for the detection of IgA deposits in skin has made such provocation tests obsolete. In addition, withdrawal of dietary gluten resulted in resolution of the skin lesions. The continual appearance and disappearance of lesions may result in hyperpigmentation and hypopigmentation. Patients may present with only crusted lesions, and a thorough search may not reveal a primary lesion. Symptoms vary considerably from the usually severe burning and itching in most patients to the almost complete lack of symptoms in a rare patient. Most patients usually can predict the eruption of a lesion as much as 812 hours before its appearance because of localized stinging, burning, or itching. The usual symmetric distribution of lesions on elbows, knees, buttocks, shoulders, and sacral areas is seen in most patients at one time or another. This patient has many firm-topped vesicles and bullae, some erosions, and residual hyperpigmentation. Direct immunofluorescence showing granular dermal papillary deposits of immunoglobulin A. The presence of C3 in both perilesional and normal-appearing skin is not affected by treatment with dapsone (diaminodiphenyl sulfone), but C3 may not be detectable after treatment with a gluten-free diet. Early studies indicated that IgA is preferentially associated with bundles of microfibrils and with anchoring fibrils of the papillary dermis immediately below the basal lamina. In addition, in such early lesions, the upper and middle dermal blood vessels are surrounded by a lymphohistiocytic infiltrate as well as some neutrophils and an occasional eosinophil. Biopsy of an early lesion showing dermal papillary collections of neutrophils and eosinophils and subepidermal vesiculation at low (A) and high (B) magnification. This is thought to occur because the lamina lucida is the most vulnerable component of the dermalepidermal junction. In addition, the distribution of the gastrointestinal lesion in the small intestine is, as a general rule, more widespread in celiac disease. In patients not taking dapsone or related drugs, the latter is usually due to malabsorption. If decreased bone mineral density is found, patients should be encouraged to begin a gluten-free diet. Strict adherence to a gluten-free diet will, after variable periods of time (from 5 months to 1 year), reduce or completely eliminate the requirement for medication in most, but not all, patients. Neurotic excoriations, eczema, papular urticaria, transient acantholytic dermatosis, pemphigoid, pemphigoid gestationis, erythema multiforme, and various other dermatoses can be differentiated easily on the basis of histologic and immunologic criteria. Linear IgA disease may be more difficult to differentiate clinically and histologically, but it is distinctive immunologically. Symptoms may abate in as few as 3 hours or as long as a few days after the first pill is taken, and new lesions no longer erupt after 12 days of treatment. This response to therapy was, for a long time, the most important element in making a diagnosis. The preferred treatment for an adult is dapsone at an initial dosage of 100150 mg/ day (this usually can be taken once a day). Patients should be instructed to take the minimal dose required to suppress signs and symptoms. Not all patients require daily treatment; in rare cases, 25 mg weekly is sufficient. Fry L et al: Effect of gluten free-diet on dermatological, intestinal and haematological manifestations of dermatitis herpetiformis. Dieterich W et al: Antibodies to tissue transglutaminase as serologic markers in patients with dermatitis herpetiformis. Viljamaa M et al: Malignancy and mortality in patients with coeliac disease and dermatitis herpetiformis: 30-year population based study. Fry L et al: Clearance of skin lesions in dermatitis herpetiformis after gluten withdrawal. J Invest Dermatol 97:175-182, 1991 8 Chapter 62:: Inherited Epidermolysis Bullosa:: M. The wound repair responses are often abnormal and can eventuate into chronic erosions, hypertrophic granulation tissue, scarring, or even invasive carcinoma. Studies of von Hebra13 were the first to distinguish pemphigus from inherited blistering and the term epidermolysis bullosa hereditaria was first suggested by Koebner. Hoffman,9 Cockayne,10 Touraine,11 Pasini,12 and Bart13 provided much of the information about subtypes of dystrophic epidermolysis bullosa. Herlitz described epidermolysis bullosa letalis,14 which was later found to be a part of the third major category of epidermolysis bullosa: the junctional form. The application of electron microscopy toward diagnosis of epidermolysis bullosa led to the studies of Pearson15 and collaborators who classified the patients not only on the basis of clinical findings but also on the existence of ultrastructural changes. A comprehensive classification of epidermolysis bullosa based on a combination of ultrastructural and clinical findings was completed in an early landmark treatise by Gedde-Dahl. These studies have led to an improved understanding of the biological basis of epidermolysis bullosa and, finally, a classification of epidermolysis bullosa based on genetic/protein defects, which provides a rational approach to specific molecular therapy.
When operative mortality is excluded gallbladder pain treatment diet aspirin 100 pills with amex, meningioma patients treated with complete resection do not seem to suffer any excess mortality when compared with age- and sex-matched controls. Additionally, estimated 5- and 10-year recurrence rates increase from 5 and 25 per cent with gross total to 40 and 61 per cent with subtotal resections, respectively. The nuclei, although elongated, retain the overall features of meningothelial cells. Transitional Meningioma As the name implies, this variant includes features of both the meningothelial and fibrous types, with syncytial islands of epithelioid cells alternating with bundles of spindled cells. Psammomatous Meningioma these essentially represent transitional meningiomas with psammoma bodies obscuring or replacing most of (a) (b) 36. This is the one subtype that at light microscopic and ultrastructural levels bears a greater resemblance to arachnoidal trabecular, rather than cap cells. The larger blood vessels are often markedly hyalinized, although smaller, capillary-type blood vessels often predominate; a vacuolated appearance may lead to confusion with haemangioblastomas. Among the vascular channels, islands of meningothelial cells can still be recognized, often with pleomorphic nuclei representing degenerative atypia. This variant often coexists with the microcystic subtype and is often associated with cerebral oedema. There is an even more striking female predominance than normally seen, with a predilection for frontal convexity or sphenoid ridge sites and for peritumoural oedema. The inclusions may be evenly distributed throughout the meningioma or concentrated in a small area. It is defined by dense infiltrates of lymphocytes and plasma cells that often obscure the intermingled meningothelial nests. Other common features that are more akin to an inflammatory process than a true meningioma include young age of onset, en plaque growth pattern, multifocality, spontaneous regressions and recurrences over multiple sites. Therefore, it is possible that the meningothelial proliferation in some cases is hyperplastic rather than neoplastic in nature. One group found that half of their 10 previously diagnosed cases qualified for the alternate diagnosis of IgG4-related meningeal disease on further workup. The scattered meningothelial cells may be hard to recognize as such and often display degenerative nuclear atypia. Atypical Meningioma Atypical meningioma is a histological diagnosis; notably, gross invasion of adjacent dura, bones and soft tissue does not warrant a higher grade, although it makes complete resection more difficult. Atypical meningiomas may arise from any of the more commonly benign histological patterns noted earlier. Based on current criteria, atypical meningiomas are more common than previously believed. Whereas older studies quote frequencies of 57 per cent, in contemporary series, they comprise 20-35 per cent of cases. For example, Perry and colleagues reported a 5-year recurrence rate of 40 per cent after gross total resection, as compared to a figure of 5 per cent in similarly treated benign meningiomas. These tumours require careful radiological follow-up; whether they should be treated with ancillary radiation therapy remains debated. Extensive interstitial and perivascular hyalinization is characteristic, occasionally forming thick amianthoid collagen fibres. Zorludemir and colleagues originally reported 14 cases with 61 per cent recurrence and 23 per cent mortality rates, Tumours of Meningothelial/Arachnoidal Cells (a) (b) 1813 36 (c) (d) (e) (f) 36. The overall pattern is lobulated and the stroma may contain a lymphoplasmacytic infiltrate. This chordoid pattern is often intermingled with foci of conventional meningioma, but may also be purely chordoid. Oncocytic Meningioma A small series of six meningiomas with marked oncocytic change was initially reported in 1997. This papillary pattern usually develops from more common meningioma subtypes; indeed, the papillary pattern predominates in only 25 per cent of cases, but may increase in prominence with each recurrence. Mitotic activity is variable, although additional high-grade features are typically found. They are unusually aggressive and have a propensity to invade, recur and metastasize. Most rhabdoid meningiomas have other features of malignancy, including high mitotic counts, cytological atypia and necrosis. However, the behaviour of focally rhabdoid meningiomas that otherwise lack malignant features remains to be determined. Such tumours should probably be graded as usual, perhaps with the patient being followed more carefully. Earlier definitions of malignancy presented considerable problems, because the association with poor prognosis was inconsistent. In contrast to prior definitions, brain invasion no longer constitutes an absolute criterion for malignancy. As such, whereas the diagnosis of atypical meningioma has increased, the more stringent definition of malignancy has led to a decrease in anaplastic meningiomas, with current estimates at 13 per cent of cases. The usual female predominance of meningiomas is not observed in malignant meningiomas. They present either as anaplastic from the outset (de novo) or via progression from atypical or benign meningiomas (secondary). It is typically found at the periphery of larger meningiomas as irregular tongue-like protrusions that incite a brisk reactive astrocytosis in adjacent brain. The previously held opinion that brain invasion is synonymous with malignancy in meningiomas is no longer tenable. The distinction between brain invasive and otherwise malignant meningiomas is further supported by molecular genetic investigations, because brain invasive meningiomas without malignant cytological features rarely harbour the genetic changes characteristic of malignant meningiomas. This pattern was originally described by Cushing and Eisenhardt in a patient who underwent 17 operations, ultimately succumbing to pulmonary Tumours of Meningothelial/Arachnoidal Cells (a) (b) 1815 36 (c) (d) (e) (f) 36.
Aspirin Dosage and Price
Aspirin 100pills
- 1 packs - $26.31
- 2 packs - $41.52
- 3 packs - $56.72
- 4 packs - $71.93
- 5 packs - $87.13
- 6 packs - $102.33
- 7 packs - $117.54
- 8 packs - $132.74
- 9 packs - $147.94
- 10 packs - $163.15
This can result in loss of the uppermost epidermis (predominantly stratum corneum) pain treatment for ovarian cysts generic 100 pills aspirin free shipping, yielding a characteristic, collarette-like depressed area that has been described as "mauserung" (molting). Mutations have been found in the gene encoding keratin 2,64 a differentiation keratin of the suprabasilar epidermis that is expressed in the more superficial epidermal layers. Keratinocytes within the granular and upper spinous layers may have perinuclear vacuolization, and some have prominent perinuclear shells. On electron microscopy, there are concentric, unbroken shells of tonofilaments surrounding the nucleus. Study of a three-generation family with ichthyosis hystrix of Curth and Macklin identified a mutation in the variable tail domain (V2) of the keratin 1 gene. Structural analyses of the resulting abnormal keratin showed a failure of keratin intermediate filament bundling, retraction of the cytoskeleton from the nucleus, and failure of localization of loricrin to desmosomal plaques. Clinical expression varies, even within families, from palmoplantar keratoderma to severe generalized involvement. There can be widespread patchy, thick, graybrown hyperkeratosis, most marked on the extensor arms and legs. In some cases, explosive bouts of widespread erythema with blisters and pustules are seen. Involvement may vary from mild to severe, but this variation has not been well characterized. During the first 2 weeks of life, the membrane breaks up and peels off, often leaving fissures, with impairment of the barrier to infection and water loss. This can lead to an increased risk of infection, difficulties in thermal regulation, and hypernatremic dehydration. These newborns usually benefit from a humidified incubator where the air is saturated with water; wet compresses followed by bland lubricants can be used to further hydrate the membrane and achieve maximum pliability. Collodion presentation can develop into a wide spectrum of ichthyotic phenotypes as the child grows (Box 49-1). The infant is 36 hours old and is covered with a macerated membrane that shows fissures; note ectropion and eclabium. In addition, an autosomal recessive, self-healing collodion baby has been described, where the skin greatly clears within the first few weeks and transitions into mildly affected or normal skin. Because there is a high frequency of new mutations, the disease may be unexpected and the diagnosis may be unknown. Epidermolysis bullosa or staphylococcal scalded-skin syndrome may be suspected, and the infant treated with antibiotics. Specialized skin care can minimize blistering and enhance healing of erosions and may include lubrication to decrease friction and mechanical trauma, protective padding, and specialized wound dressings. The newborn with extensive erosions is prone to bacterial infection and sepsis, and carefully chosen topical and systemic antibiotics can minimize the extent of infection. Infants and children may have feeding problems, with poor absorption and failure to thrive. Most patients have a specific hair shaft abnormality called trichorrhexis invaginata, in which the distal hair segment is telescoped into the proximal one, forming a ball-and-socket-like deformity on microscopic examination. This is also known as "bamboo hair" and is due to abnormal cornification of the internal root sheath. Hair from multiple areas should be examined, because only 2050% of hair may be affected; the characteristic abnormality may be more commonly observed on eyebrow hair. Atopy in these patients may manifest as atopic dermatitis asthma, or severe food allergy (particularly to nuts), and marked elevations of serum immunoglobulin (Ig) E may occur. In some patients, generalized aminoaciduria, mild developmental delay, and impaired cellular immunity may also be present. Note rudimentary ears and the distorted appearance as a result of the thick "plates" of stratum corneum. Abnormal water loss through the skin and poor temperature regulation lead to risk of fluid and electrolyte imbalance. The infants are also at risk for infection beginning in the skin, but at the same time (because of poor temperature regulation) do not show the usual signs of infection. Treatment with systemic retinoids during the newborn period can facilitate desquamation of the membrane. There is also no evidence of the lipid lamellae that form between granular and cornified cells as a result of discharge of lamellar granule contents into the intercellular space. This discovery highlights the importance of the regulation of proteolysis in the overlap between epithelial barrier function and the hypersensitivity of atopy. However, Netherton syndrome is complicated by an abnormal skin barrier, allowing increased percutaneous absorption and associated risk for systemic toxic effects. This should be considered when using topical agents such as tacrolimus, where monitoring of serum levels may be necessary,88 and topical steroids, where iatrogenic Cushing syndrome has been reported. Skin changes may evolve to orangered with brown scale, and are associated with pruritus. Extracutaneous involvement, which is variable and may be mild, includes cataracts, decreased hearing, hepatosplenomegaly with abnormal liver enzymes and fatty liver, psychomotor delay, myopathy with elevations in serum muscle enzymes, and neurologic abnormalities. Examination of peripheral blood smears shows lipid vacuoles within granulocytes, eosinophils, and monocytes, a feature that may also be present in carriers. Limb defects occur ipsilateral to the ichthyosis and range from digital hypoplasia to agenesis of the extremity. Unilateral hypoplasia can involve the central nervous system and cardiovascular, pulmonary, renal, endocrine, and genitourinary systems. The inheritance pattern is thought to be X-linked dominant, with the condition being lethal in males.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.