
Atorlip-20
General Information about Atorlip-20
High cholesterol is a situation by which the level of ldl cholesterol within the blood is greater than regular. Cholesterol is a waxy substance that is naturally produced by the liver and is also present in certain meals. It is an integral part of cell membranes and is used by the body to provide hormones, vitamin D, and bile acids. However, when the level of ldl cholesterol within the blood is simply too excessive, it can result in the formation of plaque within the arteries, which increases the danger of heart illness and stroke.
Atorlip-20, also known as Atorvastatin, is a commonly prescribed treatment for prime ldl cholesterol. This medicine is a member of a category of medication referred to as statins, which work by blocking the enzyme that produces ldl cholesterol in the liver. Atorvastatin is available in various types, however Atorlip-20 is a tablet form that incorporates 20 mg of the energetic ingredient.
People with liver illness, kidney illness, or a history of alcohol abuse ought to use Atorlip-20 with caution. It can be not beneficial for use in pregnant or breastfeeding girls. Additionally, Atorlip-20 may work together with other medicines, such as blood thinners, antibiotics, and antifungal drugs. Therefore, it is essential to tell the doctor about all of the medicines being taken earlier than beginning treatment with Atorlip-20.
Atorlip-20 is usually taken as soon as a day, with or without meals. It is necessary to observe the prescribed dosage and take the medicine on the same time every single day. Some common unwanted effects of Atorlip-20 embody headache, abdomen upset, muscle and joint ache, and diarrhea. These unwanted effects are usually mild and go away on their own. However, if they persist or become extreme, it is important to consult a well being care provider.
Atorlip-20 works by inhibiting the production of an enzyme called HMG-CoA reductase, which is responsible for producing cholesterol within the liver. By blocking this enzyme, Atorlip-20 reduces the amount of ldl cholesterol within the blood, thereby decreasing the risk of coronary heart disease and stroke. It also helps in decreasing the levels of triglycerides, a kind of fats that may also contribute to coronary heart disease.
Atorlip-20 is usually prescribed to individuals who have high ranges of LDL (bad) ldl cholesterol in their blood. LDL ldl cholesterol is the type of cholesterol that may build up within the walls of arteries and form plaque, which may slim the arteries and hamper blood move. With common use of Atorlip-20, the degrees of LDL cholesterol decrease, while the levels of HDL (good) ldl cholesterol enhance, which helps to maintain the arteries clear and reduces the chance of coronary heart disease.
In conclusion, Atorlip-20 is an efficient treatment for managing high cholesterol levels. It works by decreasing LDL ldl cholesterol and rising HDL ldl cholesterol, which helps to minimize back the danger of heart disease and stroke. However, it's crucial to comply with the prescribed dosage and inform the physician about any pre-existing conditions or medicines being taken. With correct use and monitoring, Atorlip-20 can help to improve the standard of life for people with excessive ldl cholesterol.
In addition cholesterol medication causes memory loss atorlip-20 20 mg purchase otc, an extensive capillary network beneath the epithelium in the lamina propria warms the inspired air in the conducting portion before it reaches the respiratory portion in the lungs. Type I alveolar cells, or type I pneumocytes, are extremely thin simple squamous cells that line the alveoli and are the main sites for gaseous exchange. A thin interalveolar septum with reticular and elastic fibers that is located between adjacent alveoli contains a network of capillaries. Type I alveolar cells are in very close contact with the endothelial lining of capillaries, forming a very thin bloodair barrier for gaseous exchange. The bloodair barrier consists of a thin layer of the secreted material surfactant, cytoplasm of type I pneumocyte, the fused basal lamina of the pneumocyte and the endothelial cell, and the thin cytoplasm of the capillary endothelium. They appear singly or in groups adjacent to the squamous type I alveolar cells within the alveoli. These cells synthesize and secrete a phospholipid-rich product called pulmonary surfactant. When released into the alveolus, surfactant spreads as a thin layer over the surfaces of type I alveolar cells, lowering the alveolar surface tension at the airepithelium interface. The reduced surface tension in the alveoli decreases the force that is needed to inflate alveoli during inspiration. Surfactant stabilizes the alveolar diameters, facilitates their expansion, and prevents their collapse during respiration by minimizing the collapsing forces. Surfactant also has some bactericidal effects and induces immune responses in the alveoli to counteract inhaled pathogens, fungi, viruses, and bacteria. Alveolar macrophages, or dust cells, are blood monocytes that have entered the pulmonary connective tissue septa and alveoli and function as phagocytes in both areas. The primary function of these macrophages is to clean the alveoli of invading microorganisms and inhaled particulate matter by phagocytosis. These cells are seen either in the individual alveoli or in the thin alveolar septa. They can be recognized in the alveoli or in the connective 682 tissue septa by their phagocytosed particulate or carbon particles. The serous secretory substance in which odorant molecules dissolve is produced by: A. These cells not only produce surfactant material but also can serve as stem cells for replacing type I alveolar cells during lung injury. These cells synthesize and release the tension-reducing substance surfactant for alveoli. This allows for easier alveolar expansion and prevention of alveolar collapse during respiration. These cells give rise to olfactory and supportive cells of the olfactory epithelium. The secretion from these glands contains odorant-binding proteins that bind with an odorant and is then presented to the odorant receptors on the surface of the nonmotile olfactory cilia. The kidneys are large, bean-shaped organs located retroperitoneally adjacent to the posterior body wall. Superior to each kidney is the adrenal gland embedded in renal fat and connective tissue. The concave, medial border of the kidney is the hilum, which contains three structures: the renal artery, renal vein, and the funnel-shaped renal pelvis that narrows to become the ureter. Surrounding these structures is loose connective tissue and a fat-filled space called the renal sinus. A sagittal section through the kidney shows a darker outer cortex and a lighter inner medulla, which consists of cone-shaped renal pyramids. The base of each pyramid faces the cortex and forms the corticomedullary boundary. The round apex of each pyramid extends downward to the renal pelvis to form the domelike renal papilla. A portion of the cortex also extends on each side of the renal pyramids to form the renal columns. Each renal papilla is surrounded by a funnel-shaped minor calyx that collects urine from the papilla. The minor calyces join in the renal sinus to form a major calyx that, in turn, joins to form a single funnel-shaped renal pelvis. The renal pelvis leaves each kidney through the hilum, narrows to become a muscular ureter, and descends toward the bladder on each side of the posterior body wall. Uriniferous Tubules the functional unit of each kidney is the microscopic uriniferous tubule. It consists of a nephron and a collecting duct into which empty the filtered contents of the nephron. Nephrons produce urine, and the excretory collecting ducts conduct the urine from the kidneys. The nephron, in turn, is subdivided into two components: a renal corpuscle and renal tubules. Nephrons of Kidney There are two types of nephrons, based on their location in the kidney. Cortical nephrons are located in the upper cortex of the kidney, whereas the juxtamedullary nephrons are situated near the junction of the cortex and medulla of the kidney. Although all nephrons participate in urine formation, juxtamedullary nephrons produce a hypertonic environment in the interstitium of the kidney medulla that produces concentrated (hypertonic) urine. Renal Corpuscle the renal corpuscle consists of a tuft of capillaries, called the glomerulus, surrounded by a double layer of epithelial cells called the glomerular (Bowman) capsule.
They are much more effective in preventing symptoms than reversing them once they have occurred cholesterol levels over 600 cheap atorlip-20 20 mg on-line. Allergic and inflammatory conditions H1-receptor blockers are useful in treating and preventing allergic reactions caused by antigens acting on immunoglobulin E antibody. However, the H1-receptor blockers are not indicated in treating bronchial asthma, because histamine is only one of several mediators that are responsible for causing bronchial reactions. Therefore, epinephrine is the drug of choice in treating systemic anaphylaxis and other conditions that involve massive release of histamine. They are usually not effective if symptoms are already present and, thus, should be taken prior to expected travel. The antihistamines prevent or diminish nausea and vomiting mediated by both the chemoreceptor and vestibular pathways. Meclizine is also useful for the treatment of vertigo associated with vestibular disorders. Pharmacokinetics H1-receptor blockers are well absorbed after oral administration, with maximum serum levels occurring at 1 to 2 hours. The average plasma half-life is 4 to 6 hours, except for that of meclizine and the second-generation agents, which is 12 to 24 hours, allowing for once-daily dosing. Cetirizine and levocetirizine are excreted largely unchanged in urine, and fexofenadine is excreted largely unchanged in feces. Other effects First-generation antihistamines exert anticholinergic effects, leading to dryness in the nasal passage and oral cavity. Topical formulations of diphenhydramine can cause local hypersensitivity reactions such as contact dermatitis. In addition, the first-generation antihistamines (diphenhydramine and others) with anticholinergic (antimuscarinic) actions may decrease the effectiveness of cholinesterase inhibitors (donepezil, rivastigmine, and galantamine) in the treatment of Alzheimer disease. Overdoses Although the margin of safety of H1-receptor blockers is relatively high and chronic toxicity is rare, acute poisoning is relatively common, especially in young children. Histamine H2-Receptor Blockers Histamine H2-receptor blockers have little, if any, affinity for H1 receptors. The H2-receptor blockers cimetidine, ranitidine, famotidine, and nizatidine are discussed in Chapter 40. It plays a role in vasoconstriction, inhibition of gastric secretion, and stimulation of smooth muscle contraction. Within the brain, the serotonergic neurons affect mood, appetite, body temperature regulation, and sleep. While serotonin has no therapeutic uses, selective serotonin agonists find clinical utility in the management of several disorders, such as depression and migraine headache. Location Serotonin is largely present within the enterochromaffin cells of the gastrointestinal tract. It is also found in storage granules in platelets and the raphe nuclei of the brainstem. Release of serotonin Following synthesis, serotonin is stored in vesicles and is released by exocytosis of the vesicle in response to an action potential. Serotonin has a wide range of effects that are mediated by the different types of serotonin receptors. Therapeutic Uses Selective serotonin agonists have a variety of clinical indications, depending on the receptor specificity. The clinical use of serotonin agonists in the management of migraine and obesity is further described below. Drugs Used to Treat Headache Disorders the most common types of headaches are migraine, tension-type, and cluster headaches. Patients with severe migraine headaches report one to five attacks per month of moderate to severe pain, which is usually unilateral. Headache disorders significantly affect quality of life and result in considerable health care costs. Serotonin agonists (triptans and ergot alkaloids) are effective as abortive agents in the treatment of migraines. The first, migraine without aura, is a severe, unilateral, pulsating headache that typically lasts from 2 to 72 hours. These headaches are often aggravated by physical activity and are accompanied by nausea, vomiting, photophobia (hypersensitivity to light), and phonophobia (hypersensitivity to sound). Most commonly, these prodromal symptoms are visual (flashes, zigzag lines, and glare) and occur approximately 20 to 40 minutes before headache pain begins. Women are threefold more likely than are men to experience either type of migraine. Biologic basis of migraine headaches the first manifestation of migraine with aura is a spreading depression of neuronal activity accompanied by reduced blood flow in the most posterior part of the cerebral hemisphere. This hypoperfusion gradually spreads forward over the surface of the cortex to other contiguous areas of the brain. However, the pain of both types of migraine may be due to extracranial and intracranial arterial vasodilation, which leads to release of neuroactive molecules, such as substance P, neurokinin A, and calcitonin generelated peptide. Opioids are reserved as rescue medication when other treatments for a severe migraine are not successful. The nausea that occurs with dihydroergotamine and the vasoconstriction caused by ergotamine (see below) are much less pronounced with the triptans. The onset of the parenteral drug sumatriptan is about 20 minutes, compared with 1 to 2 hours when the drug is administered orally. The drug has a short duration of action, with an elimination half-life of 2 hours.
Atorlip-20 Dosage and Price
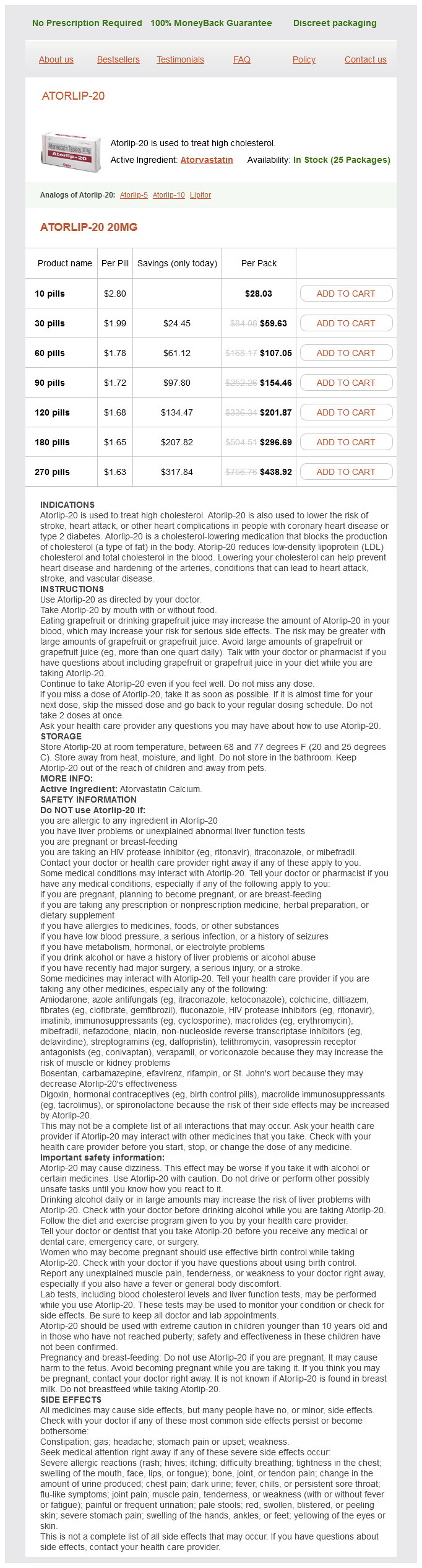
Atorlip-20 20mg
- 10 pills - $28.03
- 30 pills - $59.63
- 60 pills - $107.05
- 90 pills - $154.46
- 120 pills - $201.87
- 180 pills - $296.69
- 270 pills - $438.92
The transition zone (1) between the skin epidermis (11) and the oral epithelium is a mucocutaneous junction cholesterol medication reactions order atorlip-20 australia. The internal or oral surface of the lip is 509 lined with a moist, stratified, squamous nonkeratinized oral epithelium (8) that is thicker than the epithelium of the epidermis (11). The surface cells of the oral epithelium (8), without cornification, are sloughed off (desquamated) into the fluids of the mouth (10). Deeper connective tissue contains tubuloacinar and mucus-secreting labial glands (9, 18). The connective tissue of the lip also contains numerous adipose cells (7), blood vessels (6), and numerous capillaries. Because the blood vessels (6) are close to the surface, the color of the blood shows through the overlying thin epithelium, giving the lips a characteristic red color. The oral cavity is lined with a protective mucosa (5) that consists of an outer epithelial layer (epithelium) (5a) and an underlying connective tissue layer, the lamina propria (5b). The dorsal surface of the tongue is rough due to numerous mucosal projections called papillae (1, 2, 6). The slender, cone-shaped filiform papillae (2, 6) are the most numerous and cover the entire dorsal surface of the tongue. Less numerous are the fungiform papillae (1) with a broad, round surface of noncornified epithelium and a prominent core of lamina propria (5b). The core of the tongue consists of crisscrossing bundles of skeletal muscle (3, 7). As a result, the skeletal muscles of the tongue are typically seen in longitudinal, transverse, or oblique planes of section. In the connective tissue (9) around the muscle bundles are arteries (4a, 8a), veins (4b, 8b), and nerve fibers (11). In the lower half of the tongue and surrounded by skeletal muscle fibers (3, 7) is a section of the anterior lingual gland (10). This gland is of a mixed type and contains both mucous acini (10b) and serous acini (10c), as well as mixed acini. The interlobular ducts (10a) from the anterior lingual gland (10) pass into the larger excretory duct of the lingual gland (12) that opens into the oral cavity on the ventral surface of the tongue. The lingual epithelium (2) that covers the circumvallate papilla is stratified squamous epithelium (1). The underlying connective tissue, the lamina propria (3), exhibits numerous secondary papillae (7) that project into the overlying epithelium (1, 2) of the papilla. A deep trench, or furrow (5, 10), surrounds the base of each circumvallate papilla. The oval taste buds (4, 9) are located in the epithelium of the lateral surfaces of the circumvallate papilla and in the epithelium on the outer wall of the furrow (5, 10). The secretory product from the serous acini (6b, 11b) produces solvents for taste-inducing substances. Most of the core of the tongue consists of interlacing bundles of skeletal muscles (12). Examples of skeletal muscle fibers sectioned in longitudinal (12a) and transverse (12b) planes are abundant. This interlacing arrangement of skeletal muscles (12) gives the tongue the necessary mobility for phonating and chewing and swallowing of food. The lamina propria (3) surrounding the serous glands (6, 11) and muscles (12) also contains an abundance of blood vessels (8). The surface of this papilla (2) is covered by stratified squamous epithelium (3) that is not cornified or keratinized. The fungiform papilla (2) also exhibits numerous taste buds (4) located in the epithelium on the apical surface of the papilla, in contrast to the circumvallate papillae, in which the taste buds are located in the peripheral epithelium. The underlying lamina propria (5) projects into the surface epithelium of the fungiform papilla (2) to form numerous indentations. Surrounding the fungiform papilla (2) are the slender filiform papillae (1), whose conical tips are covered by stratified squamous epithelium that exhibits partial keratinization. The taste buds (5, 12) are embedded within and extend the full thickness of the stratified lingual epithelium (1). The taste buds (5, 12) are distinguished from the surrounding stratified epithelium (1) by their oval shapes and elongated cells (modified columnar) that are arranged perpendicular to the epithelium (1). The supporting, or sustentacular cells (3, 8), are elongated and exhibit a darker cytoplasm and a slender, dark nucleus. The taste cells, or gustatory cells (7, 11), exhibit a lighter cytoplasm and a more oval, lighter nucleus. The basal cells (13) are located at the periphery of the taste bud (5, 12) near the basement membrane. The basal cells (13) give rise to both the sustentacular cells (3, 8) and the gustatory cells (7, 11). Each taste bud (5, 12) exhibits a small opening onto the epithelial surface called the taste pore (9). The apical surfaces of both the sustentacular cells (3, 8) and the gustatory cells (7, 11) exhibit long microvilli (taste hairs) (4) that extend into and protrude through the taste pore (9) into the furrow (14) around the circumvallate papilla. The underlying lamina propria (2) adjacent to the epithelium and the taste buds (5, 12) consists of a loose connective tissue with numerous blood vessels (6, 10) and nerve fibers. In the oral cavity, taste sensations are detected by receptor taste cells in the taste buds of the fungiform and circumvallate papillae of the tongue.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.