
Azulfidine
General Information about Azulfidine
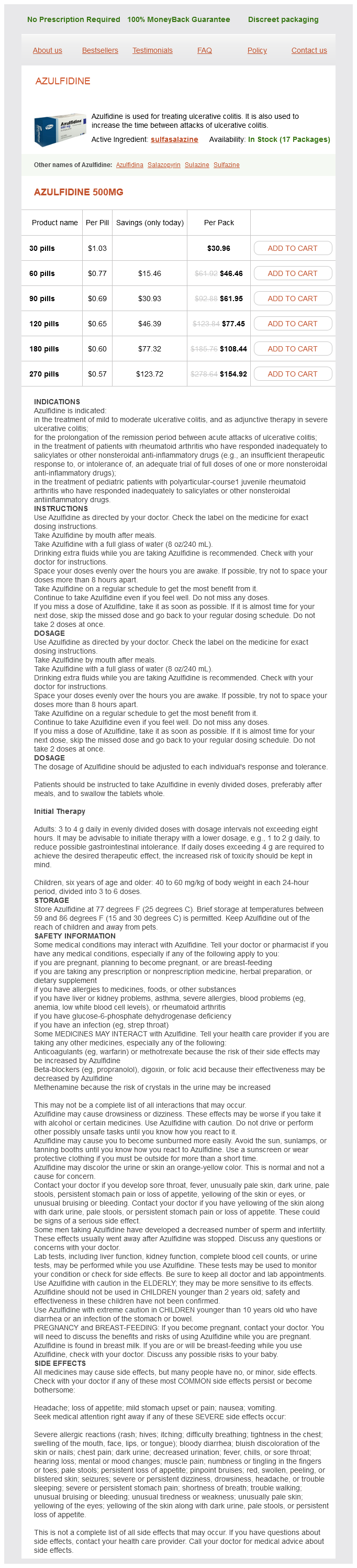
Azulfidine, also called sulfasalazine, is an aminosalicylate drug that works by reducing irritation within the colon and rectum. It is a mix of two compounds, sulfapyridine and 5-aminosalicylic acid, which work collectively to focus on totally different parts of the inflammatory process. The sulfapyridine part is responsible for suppressing the immune system, whereas the 5-aminosalicylic acid component has an anti-inflammatory impact.
Ulcerative colitis is a type of inflammatory bowel disease that causes inflammation and ulcers in the lining of the colon and rectum. It is a difficult condition to handle and may cause signs such as abdominal ache, cramping, diarrhea, rectal bleeding, and weight reduction. While the exact reason for ulcerative colitis continues to be unknown, it's believed to be an autoimmune dysfunction the place the physique's immune system attacks the healthy tissues of the digestive tract.
The use of Azulfidine has proven to have each short-term and long-term benefits for sufferers with ulcerative colitis. In the quick term, it is used to treat active irritation and supply fast relief from signs corresponding to abdominal ache and diarrhea. In the long run, it helps to scale back the frequency and severity of flare-ups, which might significantly improve a affected person's high quality of life.
While Azulfidine is an efficient therapy possibility for ulcerative colitis, like all medication, it does come with potential unwanted side effects. The most typical unwanted facet effects embrace nausea, vomiting, headaches, and loss of appetite. There can also be a potential risk of liver and kidney injury, but this is uncommon and carefully monitored by healthcare professionals.
In conclusion, Azulfidine has been a trusted and reliable medicine for the remedy of ulcerative colitis for lots of a long time. It is an important software in managing the symptoms and offering relief for these dwelling with this chronic condition. While it does come with some potential unwanted effects, the benefits of this drug far outweigh any associated dangers. With proper medical supervision and management, Azulfidine can significantly enhance the standard of life for patients with ulcerative colitis.
It is crucial to comply with the prescribed dosage and never cease taking Azulfidine abruptly, as this could result in a extreme flare-up of signs. Patients also wants to inform their physician of some other treatment they could be taking, as interactions between drugs can occur.
One of the key benefits of Azulfidine is that it can also be used as maintenance therapy to help forestall future relapses. It is very helpful for patients with delicate to reasonable illness exercise and has been proven to extend the time between attacks of ulcerative colitis.
This drug is available in pill kind and is often taken two to four occasions a day. The dosage may range relying on the severity of the situation and the individual's response to therapy. Azulfidine tablets are coated to ensure that they reach the gut before they start to dissolve. This is essential as it helps to reduce the chance of unwanted aspect effects similar to stomach irritation and discomfort.
Azulfidine is a medicine used within the treatment of ulcerative colitis, a chronic inflammatory bowel illness that affects the big intestine and rectum. Developed and marketed by Pfizer, this drug has been a staple in managing the symptoms of this situation for over 70 years.
Food is the major source of human exposure in the general population (Lagerkvist and Oskarsson nerve pain treatment uk generic azulfidine 500 mg on line, 2007). Significant amounts of vanadium are found in seafood, mushrooms, dill seed, milk, meat, cereals, and vegetables. Concentrations in rural air are much lower than in urban air, largely due to fossil fuel combustion. The dietary daily intake is estimated in the range from 10 to 60 µg (Lagerkvist and Oskarsson, 2007). The lungs absorb about 25% of soluble vanadium compounds, but the absorption of vanadium salts from the gastrointestinal tract is generally poor (Lagerkvist and Oskarsson, 2007). Some dermal absorption of soluble compounds is possible but probably represents a minor route for humans. Once absorbed, extracellular vanadium will be in the form of vanadate (5+) and most likely in the vanadyl (4+) form after entering cells. After experimental exposure by various routes in rodents, the highest amounts of vanadium are found in the bone, kidney, liver, and spleen (Lagerkvist and Oskarsson, 2007). Brain levels are considerably lower than other tissues indicating limited transport across the bloodbrain barrier. After oral exposure, vanadium shows a multicompartmental pattern with potential for accumulation and retention particularly in the bone (Lagerkvist and Oskarsson, 2007). There is some evidence that a sensitization reaction may occur with repeated exposures (Lagerkvist and Oskarsson, 2007). Gastrointestinal distress, nausea, vomiting, abdominal pain, cardiac palpitation, tremor, nervous depression, and kidney damage have also been linked with industrial vanadium exposure (Barceloux, 1999a,b). Vanadium compounds can be mutagenic in some systems (Lagerkvist and Oskarsson, 2007). Reproductive toxicology data are sparse and inconsistent, but there is some evidence of teratogenic potential in hamsters or mice (Lagerkvist and Oskarsson, 2007). There are a variety of proposed pharmacological uses for vanadium compounds, including lowering cholesterol, triglycerides, and glucose levels, and some evidence indicates it can prevent tumor growth or formation in rodents (Lagerkvist and Oskarsson, 2007). Platinum group antitumor chemistry: design and development of new anticancer drugs complementary to cisplatin. Effects of in utero tributyltin chloride exposure in the rat on pregnancy outcome. Long-term dietary cadmium intake and postmenopausal endometrial cancer incidence: a population-based prospective cohort study. Toxicity the toxicity of vanadium compounds usually increases as the valence increases, the pentavalent compounds being the most toxic. After occupational exposure to airborne vanadium, its toxic actions are largely confined to irritation of the respiratory tract, eyes, and skin (Lagerkvist and Oskarsson, 2007). Interestingly, there is usually a latent period of one to six days before the adverse effects of vanadium appear, although the effects are usually reversible. Bronchitis and bronchopneumonia are more frequent in workers exposed to vanadium compounds. Sampling and analysis considerations for the determination of hexavalent chromium in workplace air. A critical review of biomarkers used for monitoring human exposure to lead: advantages, limitations, and future needs. Age-specific fluoride exposure in drinking water and osteosarcoma (United States). Cadmium malignantly transforms normal human breast epithelial cells in to a basal-like phenotype. Skeletal changes in multiparous mice fed a nutrient-sufficient diet containing cadmium. Pulmonary response of Fischer 344 rats to acute nose only inhalation of indium trichloride. At environmental doses, dietary methylmercury inhibits mitochondrial energy metabolism in skeletal muscles of the zebra fish (Danio rerio). Lead exposure inhibits fracture healing and is associated with increased chondrogenesis, delay in cartilage mineralization, and a decrease in osteoprogenitor frequency. Biomarkers of exposure, effect, and susceptibility of arsenic induced health hazards in Taiwan. Critical exposure level of cadmium for elevated urinary metallothionein-an occupational population study in China. Efficacy of succimer chelation for reducing brain lead in a primate model of human lead exposure. Prenatal methyl mercury exposure from fish consumption and child development: a review of evidence and perspectives from the Seychelles Child Development Study. Evaluation of the cytotoxicity, genotoxicity and mutagenicity of diphenyl ditelluride in several biological models. Neurobehavioral effects of dental amalgam in children: a randomized clinical trial. Environmental distribution, analysis, and toxicity of organometal(loid) compounds. Interspecies differences in metabolism of arsenic by cultured primary hepatocytes. Baseline characteristics and the effect of selenium supplementation on cancer incidence in a randomized clinical trial: a summary report of the Nutritional Prevention of Cancer Trial. Cadmium-induced bone effect is not mediated via low serum 1,25-dihydroxy vitamin D. Developmental exposure to methylmercury elicits early cell death in the cerebral cortex and long-term memory deficits in the rat.
Jass described an attempt to systematically pull together probable prognostic indicators in to a combined staging and grading system [451] pain treatment in hindi purchase online azulfidine. In this, the degree of local invasion is combined with node involvement and two microscopic grading elements. These are peri-tumoral lymphocytic infiltrate and assessment of the advancing margin (low power) as either pushing or infiltrative. Although this system has been shown to be prognostically useful in several studies it has not achieved widespread acceptance. Tumour spread by the portal and systemic vasculature has long been recognised as the main route of development of hepatic, pulmonary and more distant metastases. These metastases may be present at the time of clinical presentation, but more commonly appear months to years after treatment of the primary lesion by surgical resection. It is assumed that, unless the original surgical excision was incomplete, clinically evident metastases grow from microscopic deposits that were undetectable at the time of primary staging and treatment. Uncertainty over the prognostic significance of venous invasion in early studies may well have been largely due to methodological differences in terms of the number and orientation of blocks selected and the use of elastic stains. More recently Foulis and colleagues have shown it to be among the most powerful of prognostic indicators. Using systematic elastin staining, fully 58% of cancers were shown to have evidence of vascular invasion. These had a significantly worse survival, irrespective of whether the invasion was intra- or extramural and venous invasion predicted the vast majority of patients who were to progress to systemic disease. It is therefore advocated that elastic staining should become part of routine pathological assessment [477,494]. The effect of tumour genetic abnormalities on prognosis the complex molecular events underlying the pathogenesis of colorectal cancer have thrown up a bewildering array of candidate markers of potential prognostic utility. A number of different antibodies to p53 have also been developed, with subtly differing staining patterns and variable relation to gene mutation. A comprehensive review has therefore, not surprisingly, concluded that there is no clear pattern of clinical relevance in the many published studies [495]. In molecular pathology it is likely that issues of technical methodology and sample selection will be crucial in ensuring that laboratories achieve comparable results. Involving pathologists is also crucial in ensuring that the samples analysed contain a suitable proportion of tumour cells, and estimation of this parameter should be included in molecular pathology reports. Where neoplastic cells constitute only a small proportion of the cellular population of a sample to be analysed, there may be a need for microdissection [496]. More recently, the importance of the gene as a predictive marker has become clear, with a significant impact on diagnostic pathology services. More global markers of genetic abnormality also have potential advantages as prognostic indicators in colorectal cancer. It is fixed by floating in formalin and subsequently inked on the underside before cutting. Pathological considerations in localised resections for colorectal cancer Advances in endoscopic and surgical technique have made it possible to locally resect colorectal neoplasms that would previously have required formal surgical excision. These lesions often do not have a preoperative malignant diagnosis and are resected as large high-risk adenomas. Occasionally there will be a local resection of a known cancer either through patient choice or because the individual is not fit for full surgical excision. Currently there is also interest in combining local resection with sentinel node mapping to better aid staging and selection for adjuvant therapy [475] but this approach has not yet been validated. The most common scenario is the detection of focal invasive cancer in a simple polypectomy and this is discussed in detail in Chapter 37. These procedures generate flat irregular specimens, the pathological assessment of which can be challenging and close clinical correlation is essential to ensure an optimum report. Once fixed, block selection must ensure thorough sampling of all margins (edge and deep) that will have been painted beforehand. Microscopic examination of cancers excised in this way is directed towards ensuring that complete excision has been achieved (usually with a microscopic clearance of at least 1 mm) and that other pathological indicators of adverse outcome are identified. Ueno and colleagues have also shown that incomplete excision, poor tumour differentiation, the presence of significant tumour budding, vascular invasion and extensive submucosal invasion are the key parameters in predicting an adverse outcome in these patients [505]. With the exception (for now) of budding, these parameters have been included in reporting guidelines for early colorectal cancers, including those identified in screening programmes [506,507]. However, an associated carcinoid syndrome is uncommon, even in the presence of liver metastases. Right hemicolectomy is warranted for all but small superficial lesions that can be completely excised endoscopically; an overall 5-year survival rate of only 23% has been reported [508]. Endocrine tumours Endocrine cell neoplasms of the large intestine, previously known as carcinoid tumours, are uncommon, accounting for less than 1% of all colorectal neoplasms, but about 30% of all endocrine cell tumours of the gastrointestinal tract [508]. In England approximately 8% of all gastrointestinal endocrine tumours arise in the rectum, whereas 13% are located in the right colon and caecum [509]. The aetiology of these tumours is uncertain, but a Swedish study has found an increased relative risk in individuals with parental carcinoid tumours, implying that genetic factors could play a role [510]. No sex difference in incidence has been noted [509] but there may be a slight increase in incidence among black and Asian populations. Endocrine cell tumours are reported to occur in patients with ulcerative colitis but there is no evidence that their incidence is increased compared with non-colitic patients [511]. Small colorectal endocrine cell tumours are discovered at endoscopy and their incidence is likely to increase with increasing endoscopy, especially for cancer screening. However, many colorectal carcinoids are incidentally discovered in resection specimens for carcinoma [512]. The most common colorectal endocrine cell tumours arise in the appendix and are considered in Chapter 30. However, published recommendations including proformas for reporting colorectal endocrine tumours are site specific, because tumours arising at different sites differ in their biology and outcomes.
Azulfidine Dosage and Price
Azulfidine 500mg
- 30 pills - $30.96
- 60 pills - $46.46
- 90 pills - $61.95
- 120 pills - $77.45
- 180 pills - $108.44
- 270 pills - $154.92
Thallium compounds back pain treatment physiotherapy buy azulfidine 500 mg low cost, chiefly thallous sulfate, were used as rat poisons and insecticides. Industrial poisoning is a special risk in the manufacture of fused halides for the production of lenses and windows. Naturally high thallium concentration in soils and consequent uptake in to edible plants in Southwest Guizhou, China, caused locally endemic chronic thallium poisoning (Xiao et al. Following the initial exposure, large amounts are excreted in urine during the first 24 hours, but after that urinary excretion becomes slow and the feces become an important route of excretion. The half-life of thallium in humans has been reported to range from one to 30 days and depends on the initial dose. Thallium can transfer across the placenta and is found in breast milk, and may cause toxicity in the offspring (Hoffman, 2000). Tellurates and tellurium are of generally low toxicity, but tellurites are typically more toxic. Acute intoxication by inhalation results in sweating, nausea, a metallic taste, and garlic smelling breath. In fact, garlic breath is an indicator of exposure to tellurium by dermal, inhalation, or oral routes. The cases of tellurium intoxication reported from industrial exposure do not appear to have been lifethreatening. Two deaths occurred within six hours of accidental poisoning by mistaken injection of sodium tellurite (instead of sodium iodine) in to the ureters during retrograde pyelography (Gerhardsson, 2007). The victims had garlic breath, renal pain, cyanosis, vomiting, stupor, and loss of consciousness. In rats, chronic exposure to high doses of tellurium dioxide produces renal and hepatic injury (Gerhardsson, 2007). Rats fed metallic tellurium at 1% of the diet develop demyelination of peripheral nerves (Goodrum, 1998), probably due to the inhibition of cholesterol biosynthesis (Laden and Porter, 2001). Tellurium compounds are genotoxic and/or mutagenic in hamster fibroblasts, fungus and bacteria (Degrandi et al. There are no data on human or animal carcinogenicity of tellurium; however, there are studies indicating an anticarcinogenic effect of tellurium (Gerhardsson, 2007). Lifetime exposure to sodium tellurite at 2 mg Te/L drinking water had no effect on tumor incidence in rats. Other signs and symptoms also occur depending on the dose and duration of exposure. Depilation begins about 10 days after ingestion and complete hair loss can occur in about one month. Other dermal signs may include palmar erythema, acne, anhydrosis, and dry scaly skin due to toxic effects of thallium on sweat and sebaceous glands. After oral ingestion of thallium, gastrointestinal symptoms occur, including nausea, vomiting, gastroenteritis, abdominal pain, and gastrointestinal hemorrhage. Neurological symptoms usually appear two to five days after acute exposure, depending on age and the level of exposure. A consistent and characteristic feature of thallium intoxication in humans is the extreme sensitivity of the legs, followed by the "burning feet syndrome" and paresthesia. Central nervous system toxicity is manifest by hallucinations, lethargy, delirium, convulsions, and coma. The acute cardiovascular effects of thallium are initially manifested by hypotension and bradycardia due to direct effects of thallium on sinus node and cardiac muscle. Major symptoms of chronic thallium poisoning include anorexia, headache, and abnormal pain. Other toxic effects of thallium include fatty infiltration and necrosis of the liver, nephritis, pulmonary edema, degenerative changes in the adrenals, and degeneration of the peripheral and central nervous system. In severe cases, alopecia, blindness, and even death have been reported as a result of long-term systemic thallium intake. A recent review on thallium poisoning during pregnancy in humans gives a range of fetal effects from severe toxicity to normal development. The only consistent effect identified is a trend toward prematurity and low birth weight in children exposed to thallium during early gestation (Hoffman, 2000). Evidence that thallium is mutagenic or carcinogenic is scanty (Leonard and Gerber, 1997). In contrast, it may be teratogenic, especially with regard to cartilage and bone formation, but most of the evidence comes from birds and not mammals. The tissue distribution of tin from these organometallic compounds shows the highest concentration in the bone, liver, kidney, and lung, with smaller amounts in the muscle, spleen, heart, or brain. Tetraethyltin, triethyltin, and diethyltin undergo dealkylation to ethyltin compounds, whereas tributyltin is dealkylated to di- and mono-butyltin compounds. Prussian blue is the recommended drug of choice in acute thallium poisoning (Hoffman, 2003). Desferrioxamine has also been tested and shown to remove thallium from the body (Fatemi et al. Tin is one of the earliest metals known and was used as a component of bronze from antiquity. Because of its hardening effect on copper, tin was used in bronze implements as early as 3500 bc. Metallic tin can combine with chloride, sulfur, or oxygen to form inorganic tin compounds (stannous, Sn2+; and stannic, Sn4+). Currently, tin is used in the manufacture of various alloys, such as bronze and brass, for fabricating window glass and in solders, but was previously widely used in food packaging. Organic tin compounds have been used in fungicides, bactericides, and slimicides, as well as in plastics as stabilizers. Bioconcentration in aquatic organisms and ecotoxicity are dependent on the bioavailability of the particular compounds.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.