
Benicar
General Information about Benicar
In conclusion, Benicar is a broadly used treatment for controlling hypertension in adults and children. With its effectiveness in bettering blood pressure and stopping associated complications, it has become a vital part of many patients' remedy plans. However, as with any medicine, it is crucial to observe your doctor's directions, monitor for unwanted effects, and discuss any considerations or potential interactions with different medicine. By working closely together with your healthcare supplier, you probably can successfully handle your blood stress and lead a more healthy life.
In uncommon instances, Benicar has been associated with a extreme situation referred to as sprue-like enteropathy, inflicting persistent diarrhea and weight loss. This aspect effect is extra common in folks of Asian descent and people taking giant doses of the medicine. If you expertise persistent diarrhea or unexplained weight reduction, converse to your physician immediately.
Benicar, also recognized by its generic name olmesartan, is a prescription medicine generally used to treat high blood pressure, or hypertension. It belongs to a class of drugs often known as angiotensin II receptor blockers (ARBs), which work by blocking the action of a hormone called angiotensin II and serving to blood vessels relax and widen, thus decreasing blood strain.
When taken regularly, Benicar helps to lower blood pressure and forestall problems related to high blood pressure. It can be used alone or in combination with different blood pressure medications, and the effectiveness of the treatment may be monitored through regular blood stress checks. In some cases, a affected person's dosage might have to be adjusted to attain the specified outcomes.
High blood pressure is a typical situation affecting tens of millions of individuals worldwide, and if left untreated, it could possibly enhance the danger of significant health problems similar to heart illness, stroke, and kidney illness. Many components can contribute to high blood pressure, together with genetics, life-style decisions, and underlying medical conditions. While life-style modifications, similar to sustaining a wholesome weight, eating a balanced diet, and exercising often, can help management blood stress, some people may have medication to achieve adequate control.
There are additionally some precautions to listen to when taking Benicar. It isn't really helpful for pregnant or breastfeeding women or individuals with a history of kidney disease or liver illness. Patients with a known allergy to olmesartan or other ARBs must also not take Benicar. Additionally, it is essential to tell your doctor of another medications you take, together with over-the-counter medicines and supplements, to keep away from attainable interactions.
Benicar is often prescribed for adults and youngsters over the age of six who have been recognized with high blood pressure. It is out there in pill form and is usually taken once a day. The dosage may differ relying on the patient's age, severity of hypertension, and different particular person factors, and it should always be taken precisely as prescribed by a physician.
As with any treatment, Benicar might trigger certain side effects, although not everyone experiences them. Common unwanted facet effects could embrace dizziness, fatigue, headache, and nausea. More serious unwanted facet effects are rare but might include allergic reactions, problem respiration, chest ache, and swelling of the face, lips, or tongue. If you expertise any of those signs, it is essential to seek medical attention immediately.
Repeated contractions "wear it out hypertension stage 1 jnc 7 benicar 40 mg order fast delivery," so to speak, and the later movements in a series become more swift and effective. Rarely, the converse is observed-where only the later movements of a series induce myotonia (myotonia paradoxica); usually this is a feature of another condition, cold-induced paramyotonia congenita (see further on). Unlike cramp, the myotonic spasm is painless but after prolonged activity, nocturnal myalgia (a pinching-aching sensation in the overactive muscles) may develop and prove distressing. Close observation reveals a softness of the muscles during rest and the initial contraction appears not to be significantly slowed. The disease as mentioned above is usually inherited as a dominant trait so that most often, other members of the family have been affected. In other cases, the myotonia becomes evident only later in the first or second decade. The muscles are generously proportioned and may become hypertrophied but seldom to the degree observed in the recessive form of the disease described further on. Despite their muscular appearance, these patients are inept in athletic pursuits as a result of the myotonia. When severe, myotonia affects all skeletal muscles but is especially prominent in the lower limbs. Attempts to walk and run are impeded to the extent that the patient stumbles and falls. Other limb and trunk muscles are also thrown into spasm, as are those of the face and upper limbs. One of the characteristic features is grip myotonia in which the patient is unable to release a handshake and must slowly open the fingers one at a time. Occasionally a sudden noise or fright may cause generalized stiffness and falling. Small, gentle movements such as blinking or elicitation of a tendon reflex do not initiate myotonia, whereas strong closure of the eyelids, as in a sneeze, sets up a spasm that may prevent complete opening of the eyes for many seconds. If the patient has not spoken for a time, there is sometimes a striking dysarthria. Arising at night, the patient cannot walk without first moving the legs for a few minutes. After a period of rest, the patient may have difficulty in arising from a chair or climbing stairs. Loosening of one set of muscles after a succession of contractions does not prevent the appearance of myotonia in another area, nor in the same ones if used in another pattern of movement. Lacking also are the narrow face, frontal balding, cataracts, and endocrine changes typical of myo tonic dystrophy that is discussed in Chap. Myotonia that is evident in infancy is far more likely to represent myotonia congenita than myotonic dystrophy, in which myotonia rarely has its onset in the first few years of life. Myotonia can also be induced in most cases by tap ping a muscle belly with a percussion hammer (percus sion myotonia). Unlike the lump or ridge produced in hypothyroid or cachectic muscle (myoedema), the myo tonic contraction involves an entire fasciculus or an entire muscle and, unlike the phenomenon of idiomuscular irritability (contraction of a fascicle in response to striking the muscle), it persists for several seconds. An electrical stimulus delivered to the motor point in a muscle induces a pro longed contraction (Erb myotonic reaction). In Thomsen disease, as in virtually all forms of myotonia, the stiffness is somewhat exaggerated in cold. On a cold day, affected individuals may have a prolonged grimace with closed eyes after a sneeze. We encountered two brothers with this disorder who described diving into a cool swim ming pool on a hot s ummer day and having to lie nearly motionless at the bottom of the pool for several seconds until the muscle stiffness abated enough to allow them to swim to the top. However, as mentioned, prominent cold-induced myotonia, is more characteristic of para myotonia congenita (see later). Biopsy reveals no abnormality other than enlarge ment of muscle fibers, and this change occurs only in hypertrophied muscles. As often happens in fibers of increased volume, central nucleation is somewhat more frequent than it is in normal muscle. In well-fixed biopsy material examined under the electron microscope, Schroeder and Adams discerned no significant morphologic changes. Myotonia levior was the name applied by DeJong to a dominantly inherited form of myotonia congenita in which the symptoms are milder and of later onset than those of Thomsen disease. The only possible exceptions are the Schwartz-Jampel syndrome of hereditary stiffness combined with short stature and muscle hypertrophy, and stiff-man syndrome which are discussed in Chap. Uncertainty in diagnosis arises in patients who have only myotonia in early life and later prove to have classic (type 1) myotonic dystrophy or who notice myotonia in adulthood with mild proximal weakness and are found to have type 2 myotonic dystrophy (see later). The most troublesome aspect of the disease is the transient weakness that fol lows initial muscle contraction after a period of inactivity. Progression of the disease continues to about 30 years of age, and according to Sun and Streib, the course of the illness thereafter remains unchanged. In paramyotonia congenita there is also In contrast myotonia of early onset, but, again, it tends to be mild, involving mainly the orbicularis oculi, levator palpebrae, and tongue; the diagnosis of paramyotonia is seldom in doubt because of the worsening with continued activity and prominent cold-induced episodes of myotonia and paralysis. In patients with very large muscles, one must con sider not only myotonia congenita but also familial hyperdevelopment, hypothyroid myopathy, the Bruck-de Lange syndrome (congenital hypertrophy of muscles, mental retardation, and extrapyramidal movement dis order), Becker myotonia (see later), Duchenne dystrophy, and most of all, hypertrophic myopathy (hypertrophia musculorum vera); this last disease is of interest because the aberrant protein (myostatin) and gene defect have been characterized. Testicular atrophy, cardiac abnormality, frontal baldness, and cataracts-the features that characterize myotonic dystrophy-are conspicuously absent. The derivative disorders normokalemic periodic paralysis, acetazolamide responsive myotonia, myotonia fluctuans, and myotonia per manens are variants of hyperkalemic periodic paralysis. All of them are caused by mutations in the gene encoding the alpha subunit of the membrane-bound voltage-gated Hyperka lemic Periodic Pa ra lysis the essential features of this disease are episodic general ized weakness of fairly rapid onset and a rise in serum potassium during attacks. Weakness appearing after a period of rest that follows exercise is particularly charac teristic. This type of periodic paralysis was first described and distinguished from the more common (hypokalemic) form by Tyler and colleagues in 195 1.
A number of them tend to be par ticularly common in certain forms of retardation: hand flapping in autism heart attack neck pain purchase 20 mg benicar with mastercard, handwringing in Rett syndrome, and hand-waving in Down syndrome and other disorders. Self-stimulation, even hurtful-such as striking the fore head or ears or biting the fingers and forearms-seems to be compulsive or perhaps to provide some sort of sat isfaction. It is not that these rhythmias are by themselves abnormal, for some of them occur for brief periods in normal babies, but that they persist. Nevertheless, many moderately delayed persons, when assigned to a simple task such as putting envelopes in a box, can continue this activity under supervision for several hours. Severe protein-calorie malnutrition in the first 8 months of life, which induces kwashiorkor, has been reported to retard mental development. The action of exogenous toxins during pregnancy is another factor to be considered. Severe maternal alco holism has been linked to a dysmorphic syndrome and developmental delay, but the findings of several studies have not been consistent (see Chap. The point to be made is that all aspects of intellectual life, personality, and deportment are affected in slightly differing degrees and that these effects have a neurologic basis. There is more than a hint that in particular diseases, because of their anatomy, the cognitive experience, affective life, and behavior are affected in special ways. The group of moderately delayed, like the severely affected ones, is divisible into groups with somatic sys temic and neurologic abnormalities, although the propor tions are not the same. There are fewer of the dysmorphic type and more of the nondysmorphic, nonneurologic group. Surprisingly, maternal addiction to opiates, while causing an opiate withdrawal in infants for weeks or even months (Wilson et al), seems not to result in permanent injury to the nervous system. The importance of exposure to extremely small amounts of environmental lead is also controversial. The effect of psychologic deprivation on cognitive development has been of interest. Orphaned and neglected babies were found to be inactive, apathetic, and backward in comparison with those who were constantly stimulated by caring mothers. But surprisingly, when nurtured properly at a later time, these babies soon caught up with their peers. This general idea of psychologic deprivation has been the basis of many interesting educational programs for poor and neglected children. To this day, however, it has not been proven that sensory, emotional, and psycho logic deprivations of a degree observed in humans are the causes of severe developmental delay or repeated scholastic failure. The controversies regarding the effects of prematurity, maternal hypertension, and eclampsia, which are often associated with neonatal cerebral pathol ogy and slowed psychomotor development, have been mentioned earlier in this chapter. The degree of developmental delay is variable, depending on the location and extent of a demonstrable neuropathology. Usually the family history is negative, but careful questioning of parents regarding the preg nancy, delivery, and early postnatal period and examina tion of hospital records from birth may disclose the nature of the neurologic insult. The third category is one in which neither somatic anomalies nor focal neurologic signs are present, or if pres ent, they are minimal. The more severely delayed in cog nitive development of this special group are represented by the following disease states: autism (Asperger-Kanner syndrome), the Rett and Williams syndromes, and the fragile X and Renpenning syndromes. All of these but autism are now known to have a genetic basis as noted earlier in the chapter and are described together below. The practical importance of this clinical approach is that it directs the intelligent use of laboratory procedures for confirmation of the diagnosis. First, as already described, there is an advantage in set ting aside as one large group those who are only mildly developmentally delayed from those who have been severely delayed in psychomotor development since early life. With regard to the former group, having no obvious neurologic signs or physical stigmata, one should nevertheless initiate a search for the common metabolic, chromosomal, and infective diseases. In this large group, one must be sure that their deficit is a general one and not one of hearing, poor sight, or the special isolated language and attention deficits. For patients with moderately severe and very severe cognitive deficits, one begins with a careful physical examination, searching specifically for somatic stigmata and neurologic signs. Abnormalities of eyes, nose, lips, ears, fingers, and toes are particularly important, as are head circumference and a variety of neurologic abnor malities, as outlined in Table 38-8. Data so obtained allow classification into one of three categories, as follows: are useful in clarifying maldevelopment and neurologic diseases but are seldom helpful in the third group of cases. A major pitfall in this clinical approach is in mistak ing a hereditary metabolic disease for a developmental one. Here one is helped by the fact that manifestations of the metabolic diseases are not usually present in the first days of life; they appear later and are progressive and often associated with specific visceral abnormalities. However, some metabolic diseases are of such slow progression that they appear almost stable, especially the late-onset ones, such as one type of metachromatic leukodystrophy, late-onset Krabbe leukodystrophy, adult adrenoleukodystrophy, and adult hexosaminidase defi ciency (see Chap. A large kindred in whom developmental delay was inher ited in an X-linked pattern was first reported by Martin and Bell in developmental delay, that Lubs, in In those with somatic abnormalities (with or without obvious neurologic signs), one assumes the presence of a maldevelopment of the brain, possibly caused by a chromosomal abnormality. The psychomotor retardation is usually severe and often nongenetic and, as a rule, has a well-defined neuropathology. Diagnosis is determined ments are numerous and diverse and are summarized in Tables by the gestalt of physical signs. At first, it was assumed that the fragile X syndrome was only an example of the Renpenning syndrome (an X-linked hereditary developmental delay in males; see below) 38-1 and 38-9; some of the main ones are described earlier in the chapter. Inevitably, one turns to the several atlases to denominate the syndromes (Holmes et al; Jones). Females are sometimes affected, but their mental function is only slightly reduced. Affected males have only mild dysmorphic features (large ears, broad forehead, elongated face, and enlarged testes) that may not become obvious until puberty.
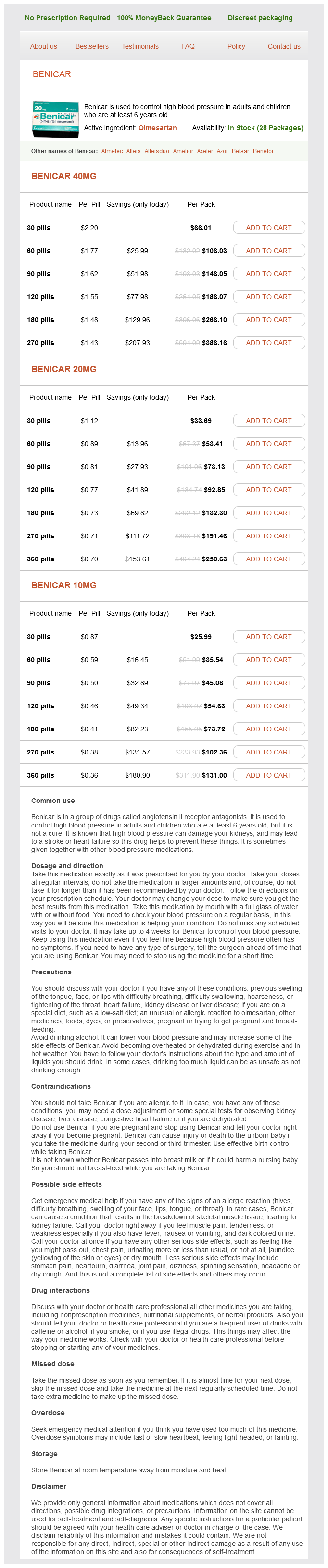
Benicar Dosage and Price
Benicar 40mg
- 30 pills - $66.01
- 60 pills - $106.03
- 90 pills - $146.05
- 120 pills - $186.07
- 180 pills - $266.10
- 270 pills - $386.16
Benicar 20mg
- 30 pills - $33.69
- 60 pills - $53.41
- 90 pills - $73.13
- 120 pills - $92.85
- 180 pills - $132.30
- 270 pills - $191.46
- 360 pills - $250.63
Benicar 10mg
- 30 pills - $25.99
- 60 pills - $35.54
- 90 pills - $45.08
- 120 pills - $54.63
- 180 pills - $73.72
- 270 pills - $102.36
- 360 pills - $131.00
There is abnormal T2 hyperintensity within the dorsal spinal cord and the cord is mildly enlarged blood pressure chart in uk buy benicar 20 mg without prescription. In the past, postinfectious myelitis was most often observed in relation to the common exanthems (rubella, rubeola, varicella). The neurologic signs appeared as the rash was fading, often with a slight recrudescence of fever. Perhaps it is advisable to do so, but there is as yet no evidence that this alters the course of the illness. We have also used plasma exchange or intravenous immune globulin in several patients with uncertain results, although this approach was seemingly helpful in a few patients who had an explosive clinical onset. Invariably, the myelitic disease improves, sometimes to a surprising degree, but there are examples in which the sequelae have been severe and permanent. Pain in the midthoracic region or an abrupt, severe onset usually indicates a poor prognosis (Ropper and Poskanzer). The authors have several times given a good prognosis for long-term recovery and assurance that no relapse will occur, only to witness a recrudescence of other symptoms at a later date, indicating that the original illness was probably multiple sclerosis. Mycoplasma is almost unique in being a bacterial trigger of the disease, but as noted earlier, there is some uncer tainty regarding its ability to cause direct infection rather than a postinfectious immune reaction. Our interpretation of the existing information still favors a postinfectious etiology. In most instances of postinfectious myelitis, the connection to a preceding infection is presumed but can not be proved. However, the clinical manifestations of the former tend to evolve more slowly, over a period of Campylobacter jejuni, which 1 to 3 weeks or even longer. Also, a rela has not led to myelitis and is a frequent precedent to acute polyneuropathy. More difficult to understand are the large number of cases of myelitis, including autopsy-proven ones, in which the disease develops without an apparent ante cedent infection. There is understandable uncertainty in such cases as to whether the illness is the opening phase of multiple sclerosis of the type described below under "Acute Demyelinating Myelitis of Multiple Sclerosis. The most typical of clinical expression of demyelinat ing myelitis is with numbness that spreads over one or both sides of the body from the sacral segments to the feet, anterior thighs, and up over the trunk, with coin cident but variable and usually asymmetric weakness and then paralysis of the legs. The differential diagnosis of demyelinating myelitis is considered more fully in Chap. Further discussion of relapsing myelitis, sometimes but acute transverse myelitis in relation to other demyelinat ing diseases can be found below and in Chap. Other patients, how ever, show no apparent response, and a proportion of cases have even continued to worsen while the medica tion was being given. Plasma exchange and intravenous immune globulin have reportedly been beneficial in individual cases, particularly in those with an explosive onset (see later). The neurologic signs may erupt so precipitously that a vascular lesion is assumed. In most other cases, the disease evolves at a slower and usually stepwise pace, over several months or years. Necrotizing myelopathy is distinguished from the more common types of transverse myelitis by a persistent and profound flaccidity of the legs (or arms if the lesion is cervical), areflexia, and atonicity of the bladder-all reflecting a widespread necrosis that involves both the gray and white matter of the spinal cord over a considerable verti cal extent. This clinical picture is unexpected for a spinal cord lesion and, therefore, is often mistakenly attributed to spinal shock or to a completely different process such as Guillain-Barre syndrome. This combination of spinal cord necrosis and optic neuritis corresponds to the syndrome described by Devic in 1894 and named by him neuromyelitis optica (Devic disease). The antibody is directed against the aquaporin channel in capillaries of the brainstem and cerebellum and its role in the pathogenesis of the disease partially resolves the decades old uncertainty regarding a distinc tion between Devic disease and forms of multiple sclero sis, in which the antibody is not present. Imaging studies performed weeks or more later show atrophy of the involved segments of cord. Note the long extent of the lesion and thinning of the cord as the acute illness subsides. In cases coming to postmortem examination at vari able times after the onset of symptoms, the lesion has proved to be a necrotizing myelitis with widespread loss of spinal cord tissue. However, areas of residual inflammation and demyelination are often detected at the edges of the destructive lesions. Older lesions leave the spinal cord cavitated or collapsed over a vertical extent of 5 to 20 em, with conical extensions of necrosis into the gray matter above and below the area of transverse damage. Probably many of these cases would now be categorized as part of the neuromyelitis family with aquaporin autoantibodies. The veins are also thickened and surrounded by lymphocytes, mononuclear cells, and macrophages. These findings have been difficult to interpret and their relationship to the group of arteriovenous malfor mations and fistulas, discussed later, has been unclear but we are inclined to the view of Antoni and others who were impressed with the prominence of large arteries and veins and have reinterpreted this pathologic process as an arteriovenous malformation. The spinal fluid formula has also varied but generally does not con tain oligoclonal bands. Treatment with prednisone and cyclophosphamide or methotrexate has been suggested and was seemingly successful in several of our patients. There is little pathologic material on which to judge the association, but the presence of other infl ammatory lesions of the central and peripheral nervous system in Sjogren disease makes the existence of myelitis plausible. A similar syndrome is produced by a rare idiopathic necrotizing vasculitis that is confined to the spinal cord (Caccamo et al). In these cases, there is a persistent and marked pleocytosis and some clinical stabilization with corticosteroids. One of our young male patients with this type of subacute necrotizing myelitis, responsive to corticosteroids, had mononuclear cells in the spinal fluid persistently over a year and died as a result of fulminant infl ammatory cerebral hemorrhages. There were multiple occlusions of small vessels surrounding the spinal cord and a vasculitis. Polyarteritis nodosa and necrotizing arte ritis only rarely involve the spinal cord.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.