
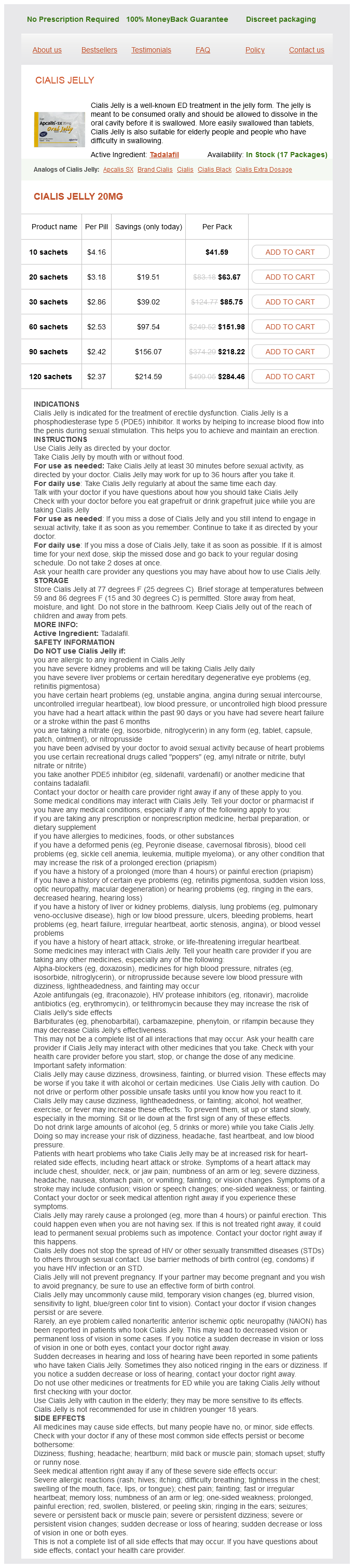
Cialis Jelly
General Information about Cialis Jelly
It is price noting that Cialis Jelly is not an aphrodisiac and will not cause an erection without sexual stimulation. It additionally doesn't protect in opposition to sexually transmitted ailments, and it's important to observe safe sex practices at all times.
As with any treatment, there could additionally be some side effects associated with Cialis Jelly, similar to headache, dizziness, and upset abdomen. These unwanted facet effects are usually delicate and temporary, but when they persist or become severe, it is essential to seek medical attention.
Erectile dysfunction (ED), also known as impotence, is a standard situation that affects many men. It is characterized by the shortcoming to attain or preserve an erection enough for sexual intercourse. While there are numerous remedies out there for this situation, some of the popular and efficient choices is Cialis Jelly.
Another distinctive good factor about Cialis Jelly is its range of flavors. From fruity to minty, there is a broad variety of options obtainable to swimsuit different tastes. This can make the expertise of taking this treatment more pleasant and pleasant, taking away the anxiety and embarrassment that may include conventional ED treatments.
In conclusion, Cialis Jelly is a broadly known and efficient ED therapy within the type of a jelly. It offers a faster absorption fee, ease of consumption, and a spread of flavors that make it a well-liked alternative among males. However, it is essential to seek the guidance of with a well being care provider before utilizing this or another medication to make sure it is safe and suitable for an individual's specific needs.
The lively ingredient in Cialis Jelly is Tadalafil, the same ingredient discovered within the traditional type of the medication. Tadalafil works by relaxing the blood vessels within the penis, permitting for increased blood flow and thus, an erection. Cialis Jelly is simply as effective as the capsule form, if no more so, as a result of its faster absorption price.
One of the main advantages of Cialis Jelly is that it might be absorbed extra shortly by the body. Unlike conventional tablets, which have to be swallowed complete and then digested, the jelly is meant to be taken orally and allowed to dissolve within the mouth. As a outcome, it could possibly provide sooner outcomes, with some males reporting an erection within quarter-hour of consumption.
One of the largest challenges for aged males or those with problem in swallowing is taking traditional tablets. Often, they could need to crush or reduce the tablets, which is normally a trouble and may have an effect on the effectiveness of the medicine. With Cialis Jelly, that is no longer a priority. The jelly is simple to swallow and dissolves rapidly, making it an ideal possibility for these people.
Cialis Jelly is a medication used to deal with erectile dysfunction in males. It comes within the type of a deliciously flavored jelly, making it a extra handy and enjoyable choice for people who battle with conventional pills. This distinctive form of medicine has gained popularity among men of all ages because of its effectiveness and ease of consumption.
Nonetheless erectile dysfunction fact sheet buy cheap cialis jelly 20 mg on line, most (68%) did not sublux even with a fracture fragment greater than 39%. Giddins58 has shown that the risk of subluxation can be assessed by a lateral hyperextension radiograph performed within 1 to 2 weeks of injury. The presumption is that there has not been so much volar plate and collateral ligament injury that subluxation will occur. This appears to be a variant on gliding and is not typically associated with subluxation. Together these recent papers establish that basing treatment on a fracture fragment greater than one-third of the base of the distal phalanx is unreliable in predicting subluxation. Rather a combination of a fracture fragment greater than 39%, displacement, and particularly the response to hyperextension testing should indicate the very small number of patients who require surgery to prevent appreciable, that is, long-term symptomatic, subluxation. The vast majority of patients with these injuries should do well with splintage for about 4 weeks (even that may be longer than is necessary). The two common injuries are dorsal fracture subluxations/dislocations and pilon fractures. Stable injuries, particularly fracture subluxations, with a fracture of the base of the middle phalanx of less than one-third on the lateral radiograph or pilon fractures without too much displacement appear to do well with nonoperative treatment. While many patients achieve good results with surgical treatment, there are some very poor results especially if a postoperative infection occurs. Recent work that I have done suggests that lateral flexion radiographs (comparable to the lateral extension radiographs in the assessment of stability in bony mallet injuries) can predict the injuries that need surgery and those that do not. I have not thought it "ethical" to treat the fingers that pivot, nonoperatively, in order to assess whether surgery would have been needed so I can only report on the fingers that glide. I recommend careful and regular review for a minimum of 3 weeks from injury, with repeat radiographs to ensure there is no further late collapse of the fracture and to ensure that good early mobilization occurs. I believe that the aim of treatment of intra-articular hand fractures is not primarily reduction of the fracture to a certain angle but restoration of gliding with acceptable alignment. They reported that all had persistent pain, which largely resolved with surgical stabilization. Nineteen of the 30 patients who completed questionnaires reported no pain; all 30 reported being satisfied by their treatment and none had had to change their jobs. Of the 20 patients assessed in person, there were no statistically significant reductions in pinch or grip strength, but 2 patients had some instability on stress testing. The authors reviewed the radiographs of 20 patients; they reported a nonunion rate of ¼ (5 of 20). The patients were treated with immobilization in plaster for 6 weeks and thereafter followed up for a mean of 2. Twenty-six of the 28 patients had no pain at rest or on movement and all 28 patients had the same pinch and grip strength as their contralateral uninjured side, yet 60% had radiological evidence of persistent nonunion of the avulsion fracture fragment. It is highly likely this is an injury with subtypes requiring different treatment; some of these injuries may do appreciably better treated surgically while the majority may not. This remains unproven, but it would in part explain the dichotomy between the advocates of nonoperative and operative treatment. As there is no adductor hood to give a Stener-type lesion, nonoperative treatment should give good results, that is, immobilization in plaster or a splint for 4 to 6 weeks. Despite this, surgical treatment of these injuries has been debated for a long time. This may skew the clinical impression of treatment outcome in shorter-term reviews. The optimal treatment for each subgroup is not yet established, but again nonoperative treatment should be presumed to be the management of choice for the large majority of these injuries. The long-term assessment of pain could be compared for 645 patients: 75 of 224 (33%) patients treated nonsurgically had pain at final review (mean time 12, range 626 years), compared with 73 of 421 (17%) treated surgically (mean time 5, range 211 years) (p < 0. One hundred and twenty of 122 (98%) patients treated nonsurgically returned to their previous employment at a mean of 11 (range 226) years, compared with 351 of 352 (99%) of those treated surgically at a mean of 6 (range 112) years. Radiological evidence of osteoarthritis was reported in 839 patients: 99 of 299 (33%) patients treated nonsurgically had osteoarthritis at a mean of 8 (range 226) years, compared with 182 of 540 (33%) patients treated surgically at a mean of 4 (range 112) years. Data on complications of treatment were available for 956 patients; only 2 of 287 (< 1%) of patients treated nonsurgically had complications compared to 88 of 669 (13%) treated surgically; 56 patients treated surgically required a second operation for removal of metalwork, primarily prominent tension band wires (p = 0. The quality of the data is not high, nonetheless, it seems that patients are more likely to suffer long-term pain following nonsurgical treatment and much more likely to suffer complications with surgical treatment. Despite this relatively poor treatment by current standards, 11 of the 17 had no or mild pain and 16 of the 17 had returned to their previous employment at the final review. Furthermore, although this paper has the longest follow-up, when degenerative changes may be expected to lead to symptoms, their results are not significantly different in terms of pain and function to similar conservative studies and perhaps more importantly to several of the operative studies. Surgeons should aim to achieve and hold an adequate reduction of the fracture until bone union. Thus, many of these injuries can be treated nonoperatively and an adequate reduction achieved and maintained. Ultimately, one or more randomized controlled trials comparing nonsurgical or surgical treatments are required to advance the treatment of this common injury. In addition, the quality of postoperative care such as regular review of radiographs is rarely described despite its importance in assessing and maintaining fracture alignment in the first few weeks following injury. For some injuries, surgery is rarely likely to be required, for example, spiral metacarpal fractures.
It is metabolized by cytochrome P450 in the liver sleeping pills erectile dysfunction cheap cialis jelly 20 mg buy line, then excreted in the feces (75%) and urine (14%). The most common adverse effects of fosamprenavir include nausea and vomiting, diarrhea, headache, and mild to moderate rashes. There is the less common chance that serious rashes may develop, including Stevens-Johnson syndrome, which can be fatal. Fosamprenavir may also cause hyperglycemia, newly occurring diabetes, worsening of existing diabetes, fat maldistribution, bone loss, hyperlipidemia, elevated transaminase, and increased bleeding (in hemophiliacs). ChapTer sevenTeen Antiviral Agents 277 What are the contraindications and interactions Fosamprenavir is contraindicated with cisapride, alprazolam, triazolam, midazolam, bepridil, ergot alkaloids, simvastatin, lovastatin, rifampin, and the herbal supplement St. It may also interact with oral contraceptives, so alternate forms of contraception should be used while taking fosamprenavir. Patients must be informed that fosamprenavir may cause abdominal or back pain, as well as pain in the groin or testicles. They should report these symptoms to their physician, and the drug should be temporarily or permanently discontinued. Indinavir Indinavir (Crixivan) is administered on an empty stomach, with which it has 65% bioavailability. It must not be administered with meals high in calories, fats, or proteins due to significantly decreased absorption. Patients can reduce risk of kidney stones by consuming at least 48 ounces of water daily. Additional adverse effects include newly developing diabetes, hyperglycemia, worsening of existing diabetes, fat maldistribution, bone loss, hyperlipidemia, elevated transaminase levels, and increased bleeding in hemophiliacs. Indinavir is contraindicated in hypersensitivity to any of its components, and the drugs alfuzosin, amiodarone, dihydroergotamine, ergonovine, ergotamine, methylergonovine, cisapride, lovastatin, simvastatin, pimozide, sildenafil, oral midazolam, triazolam, and alprazolam. Drug interactions with indinavir may occur with buffered didanosine, rifampin, rifabutin, ketoconazole, and the herbal supplement St. Patients must be instructed about the many medications that can cause life-threatening adverse effects if taken with indinavir. They must tell their physician about all medications they are using concurrently and not to change doses or medication schedule without notifying their physician. Though generally well tolerated, the major adverse effect of indinavir is kidney stones or nephrolithiasis, which causes flank pain, and may cause hematuria. This usually does not affect kidney function and resolves with Lopinavir/Ritonavir this fixed-dose combination, marketed as Kaletra and Aluvia, is approved for adults and children over 6 months old. Lopinavir is the active retroviral; ritonavir is included to increase its effects by inhibiting cytochrome P450. The lower levels of ritonavir mean that this component is insufficient to have significant antiretroviral effects. While the actions of ropinavir are explained in detail under its section below, lopinavir is absorbed better when taken with food. In this combination drug, lopinavir achieves much higher concentrations than ritonavir, yet is effective at much lower concentrations. Drug interactions with lopinavir/ritonavir include clarithromycin, ketoconazole, itraconazole, rifabutin, sildenafil and similar erectile dysfunction drugs, cisapride, flecainide, propafenone, dihydroergotamine, ergonovine, ergotamine, methylergonovine, pimozide, midazolam, triazolam, lovastatin, and simvastatin. Additional interactions may include methadone, ethinyl estradiol, rifampin, efavirenz, nevirapine, phenobarbital, phenytoin, carbamazepine, disulfiram, metronidazole, and the herbal supplement St. Lopinavir/ritonavir is extremely well tolerated, with the most common adverse effects being diarrhea and nausea. There are risks for new-onset diabetes, hyperglycemia, worsening of existing diabetes, fat mal-distribution, bone loss, hyperlipidemia, elevated transaminases, and increased bleeding in hemophiliacs. Additionally, the oral solution formulation of this combination drug has caused serious cardiac, renal, and respiratory problems in newborns, leading to fatalities. It should be avoided in full-term infants for the first 14 days following birth and in preterm infants until 14 days after their predicted due date. Patients must be aware of hypersensitivity reactions to this combination drug, as well as the medications to avoid taking during therapy. It is extensively metabolized in the liver and 99% is excreted in the feces, with the remainder in the urine. This drug may also cause hyperglycemia, newly occurring diabetes, worsening of existing diabetes, fat maldistribution, bone loss, hyperlipidemia, elevated transaminase, and increased bleeding (in hemophiliacs). It may also interact with ethinyl estradiol, norethindrone, rifampin, rifabutin, and the herbal supplement St. Nelfinavir is administered orally, and its absorption is doubled or tripled when taken with food. Patients must be instructed about life-threatening adverse effects that may occur if nelfinavir is taken ChapTer sevenTeen Antiviral Agents 279 with many other drugs. They must tell their physician about all medications they use, including vitamins and herbal products. It is important not to start any new medication without discussing this with their physician. Adverse effects are reduced by beginning therapy at lower dosages and titrating them upward to the maintenance dosage.
Cialis Jelly Dosage and Price
Cialis Jelly 20mg
- 10 sachets - $41.59
- 20 sachets - $63.67
- 30 sachets - $85.75
- 60 sachets - $151.98
- 90 sachets - $218.22
- 120 sachets - $284.46
Diuretics are indicated for edema (cerebral erectile dysfunction age 18 buy genuine cialis jelly on-line, acute pulmonary edema or congestive heart failure), hepatic cirrhosis with or without ascites, use with corticosteroids or estrogen therapies, acute glomerulonephritis, hypercalcemia, nephrotic syndrome, and chronic renal failure), various seizures, for the reduction of intraocular pressure in glaucoma, acute high-altitude sickness, and hypertension (including the reversal of fluid retention caused by some antihypertensive drugs) 548 UniT foUr Effects of Drugs on Specific Systems objective 8: classify the five major types of diuretics. Osmotic diuretics: affect the capacity of the renal tubule to reabsorb electrolytes and nonelectrolytes Carbonic anhydrase inhibitors: stop the conversion of carbon dioxide to carbonic acid and bicarbonate ions Thiazide and thiazide-like diuretics: inhibit sodium reabsorption on distal convoluted tubules and collecting ducts Loop diuretics: work on the loop of Henle to inhibit sodium and chloride reabsorption Potassium-sparing diuretics: decrease potassium and hydrogen ion excretion objective 9: Describe the mechanism of action for osmotic diuretics. Decrease solute content, resulting in less water reabsorption from the descending loop of Henle and collecting duct and less sodium chloride reabsorption in the proximal tubule and ascending loop of Henle objective 10: list the major adverse effects of potassium-sparing diuretics. Drugs Used to Treat Endocrine Conditions Chapter Objectives After completing this chapter, you should be able to: 1. Describe conditions linked to excessive or insufficient amounts of growth hormone. This article focuses on hormones that regulate growth, blood glucose, and intermediary metabolism. The synthesis and secretion of many hormones are controlled by other hormones or changes in the concentration of essential chemicals or electrolytes in the blood. The interrelationships among the peptide hormones of the hypothalamus, the trophic hormones of the anterior pituitary, and other endocrine glands are examples of elegant feedback regulation-positive feedback, in which one hormone stimulates the secretion of another, or negative feedback, in which one hormone turns off the action of the previous hormone. Drugs and diseases can modify hormone secretion as well as specific hormone effects at target organs. Pharmacologic preparations are used to detect and treat disorders involving any of the following glands: pituitary, thyroid, adrenal cortex, pancreas, or gonads. The effects of these drugs are derived from the physiological actions of the endogenous hormones that they stimulate if they are activators (agonists) or block if they are antagonists. Pituitary Gland the pituitary gland-sometimes called the master gland because of its regulatory effects on the other endocrine glands-consists of an anterior lobe (adenohypophysis) and a posterior lobe (neurohypophysis) that are under the influence of the hypothalamic hormones. The hypothalamic hormones control the secretion of specific trophic hormones; they in turn regulate other endocrine gland secretions and target tissues. Table 32-1 lists the pituitary gland and other endocrine glands and their functions. Clinically, an abnormal level of activity of the pituitary gland causes two conditions: hyperpituitarism-overactivity of the pituitary gland (causing gigantism or acromegaly)-and hypopituitarism-underactivity of the pituitary gland (causing dwarfism). The relationships between hypothalamic hormones, pituitary hormones, and target organs are shown in Table 32-2. The increase in length is especially prominent in bone growth, but its effect is manifested in nearly all the tissues of the body. Endocrine System the endocrine system secretes hormones that control the body by maintaining its internal environment within certain narrow ranges, which is known as homeostasis. The maintenance of homeostasis involves growth, maturation, reproduction, metabolism, and human behavior. Responsibility for homeostasis is shared by the endocrine system and the nervous system, working in tandem in a unique partnership. The hypothalamus of the brain (a part of the nervous system) sends directions via chemical signals (the releasing of hormones) to the pituitary gland (a part of the endocrine system). It stimulates the growth of the adrenal gland cortex and the secretion of corticosteroids. This syndrome is signified by a pad of fat developing between the shoulders, producing a "buffalo hump," and the face becoming round and moon shaped. Other effects in humans include the increase in testicular steroidogenesis and the development of the male accessory sex organs. Neither is made in the posterior pituitary; rather, they are synthesized in neurons in the hypothalamus. Vasopressin is used mainly for its antidiuretic effects in this disease rather than for its vasoconstrictor actions, from which the name vasopressin is derived. It plays a significant role in concentrating urine oxytocin Oxytocin stimulates the contraction of smooth muscle in the uterus and alveoli of the lactating breast. The hormone enhances uterine contractions during labor and stimulates the release of milk during breastfeeding. What are the effects of hypothalamic hormones upon trophic hormones, and what do these hormones regulate Thyroid Gland the thyroid gland lies in the neck just below the larynx and in front of the trachea. Iodine is vital for the synthesis of these hormones and is provided through the dietary intake of common iodized salt. Another hormone releases from parafollicular cells in the thyroid gland-calcitonin-which is involved with calcium homeostasis. Calcitonin inhibits bone reabsorption and the release of calcium ions into the blood while promoting the uptake of these ions back into bone. In the absence of the thyroid gland and thus thyroid hormones, the basal metabolic rate is less than half its normal rate, and growth and development are impaired. In the presence of a hyperactive gland, the metabolic rate is much higher than normal, resulting in tachycardia, nervousness, and other symptoms. A goiter can also be caused by constant stimulation of an underactive or nonfunctioning thyroid to release more hormones. Focus on Geriatrics Myxedema Coma M yxedema coma is a medical emergency that is indicated by a diminished level of consciousness associated with severe hypothyroidism. Symptoms include hypothermia without shivering, hypoventilation, hypotension, and hypoglycemia.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.