
Cytotec
General Information about Cytotec
NSAIDs, which embody over-the-counter drugs like aspirin and ibuprofen, are generally used to alleviate irritation, ache, and fever. However, they'll also trigger damage to the abdomen lining, resulting in the formation of ulcers. These ulcers can be painful and in extreme circumstances, can even cause bleeding and perforation of the abdomen, which may be life-threatening. This is where Cytotec comes in - by stopping the formation of abdomen ulcers, it protects patients from the potential unwanted effects of NSAIDs.
Apart from defending against NSAID-induced ulcers, Cytotec can be used to prevent ulcers in sufferers who are at a high threat of developing them because of conditions like rheumatoid arthritis, osteoarthritis, and ankylosing spondylitis. These conditions could cause chronic ache and inflammation, and patients could require long-term use of pain-relieving drugs to handle their symptoms. However, the extended use of those drugs can lead to abdomen ulcers, and Cytotec could be prescribed as a preventative measure to attenuate the danger.
Cytotec works by rising the manufacturing of mucus in the abdomen, which helps protect the abdomen lining from the irritative results of NSAIDs. It also reduces the manufacturing of abdomen acid, which additional helps in preventing the formation of ulcers. This makes it an efficient medicine for patients who require long-term use of NSAIDs for his or her medical situations.
In uncommon instances, Cytotec may cause severe side effects, such as allergic reactions, issue respiratory, and irregular heartbeat. It is essential to hunt instant medical attention if any of those symptoms occur. Cytotec can also be not recommended for pregnant women, as it could cause uterine contractions and lead to incomplete abortion or miscarriage.
Like any medication, Cytotec additionally has its share of potential unwanted effects. The most typical ones embody diarrhea, stomach pain, and cramps. Some patients may also expertise nausea, vomiting, and bloating. These unwanted aspect effects are usually delicate and short-term, and they often subside inside a few days of beginning the medicine. However, if they persist or turn into extreme, it is essential to seek the guidance of a physician.
In conclusion, Cytotec is a valuable medicine for stopping stomach ulcers in sufferers treated with NSAIDs or those that undergo from arthritis or persistent ache. It offers a safe and effective approach to handle the risk of ulcers and permits patients to proceed their pain management therapy with out worrying about potential stomach injury. However, it is essential to use it as directed and to consult a doctor if any unwanted effects occur. With accountable and knowledgeable use, Cytotec can present much-needed reduction to sufferers affected by circumstances that require long-term use of pain-relieving medicine.
Cytotec is often taken orally, within the form of tablets, both with meals or after meals. It is also generally prescribed together with NSAIDs, as a single medication generally recognized as Arthrotec. The beneficial dosage is dependent upon the individual's medical situation, age, and response to therapy, and it is essential to observe the doctor's instructions fastidiously.
It is essential to note that Cytotec ought to only be used for its approved medical functions. There have been reviews of individuals utilizing it off-label for inducing labor or terminating pregnancies, which might have critical and even fatal penalties. This is why it's strictly regulated and will only be used beneath a physician's supervision.
Cytotec, also identified by its generic name Misoprostol, is a medicine that has been in use for almost three decades to prevent the formation of stomach ulcers in patients handled by NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) or who suffer from arthritis or chronic pain. It is an artificial prostaglandin E1 analogue that was originally permitted by the FDA (Food and Drug Administration) in 1988 to be used as an anti-ulcer medicine.
Adverse Effects: Adverse effects of albumin administration are rare; these include changes in vital signs (heart rate treatment 5th metatarsal shaft fracture cytotec 100 mcg purchase, blood pressure and respiration), nausea, fever/chills, and allergic reactions. Furthermore, because negatively-charged albumin binds calcium, administration can lead to hypocalcemia and related complications. Albumin solutions may also contain trace amounts of aluminum, which can cause toxicity in infants and in patients with chronic renal failure. Because albumin acts to increase osmotic pressure, rapid infusion can lead to significant shifts in intravascular volume, and resultant circulatory overload (including pulmonary edema) is possible. Cost and Usage: the choice of replacement fluid has considerable cost implications. Albumin is over 30 times more expensive than crystalloid, and is often used in situations where randomized control trials have not shown a difference in patient mortality. Similar trends have also been reported in Europe, which has initiated the development of guidelines for colloid administration. Manufacturing: Although recombinant albumin is presently under study, current preparations of albumin solutions are purified from human sources (manufactured from either whole blood or plasmapheresis donations). Additionally, the product contains non-albumin proteins (<4%), endotoxins, trace metals. The manufacturing process includes steps to prevent transfusion-transmitted diseases, including heat treatment. While processing does reduce the risk of contamination, the risk of microbial contamination does still remain. In fact, seven patients developed Pseudomonas bacteremia after receiving albumin from the same lot in the 1970s. Storage: Albumin is stored at room temperature in either glass or specialized plastic containers for up to 2 years. Albumin solutions are inspected for turbidity by the manufacturer, and prior to use as a quality control measure to detect potential bacterial contamination. Typically, 5% albumin expands the volume equal to the volume of albumin infused; whereas 25% albumin will expand the volume by 3. Thus, if 25% albumin is used in dehydrated patients, additional fluids are indicated to avoid further exacerbating dehydration of tissues. It is possible to dilute 25% albumin, but it must be diluted with normal saline only. Dilution with sterile water can lead to hemolysis red blood cells due to hypotonicity, and has resulted in death. Smaller doses may also be diluted with 5% dextrose Albumin and Related Products 241 in water (D5W), but large volumes of D5W-diluted albumin may lead to hyponatremia with resultant sequelae, including cerebral edema. Clinical factors surrounding fluid status should guide product choice in the context of the above considerations. Albumin Dosing: Adult Dosing: A typical initial adult dose is 25 g, which may be repeated after 1530 minutes, dependent upon the patient response. In a 48-hour period, a maximum of 250 g of albumin can be infused; however, no standard dose of albumin is applicable to all clinical situations, and clinical parameters must be used to determine appropriateness of response. Infusion rates vary depending on the albumin concentration to prevent complications of rapid volume expansion; as a guideline, 5% albumin solutions are started at a rate of 12 ml/min and increased to a maximum rate of 4 ml/min, while 25% albumin solutions are not infused at rates >1 ml/min. Pediatric Dosing: Dosing in pediatrics is dependent on the clinical indication for administration. Other Colloid Solutions: Alternatives to albumin for plasma expansion include crystalloids. Crystalloids and non-protein colloids have not demonstrated a benefit over albumin, but are less expensive. Non-protein colloids have been associated with side-effects, including coagulopathy, pruritis, and head and back pain. Dextrans: Dextran is a synthetic colloid consisting of a mixture of glucose polymers derived from the action of Leuconostoc mesenteroides on sucrose, and is currently available in 10% dextran 40 (40 kDa) and 6% dextran 70 (70 kDa) formulations. Dextrans have a high water-binding capacity; for example, 1 g of dextran 40 retains 30 ml of water, while 1 g dextran 70 retains 2025 ml of water. Dextran is mostly eliminated by the kidneys and, as a result, should be avoided in patients with impaired renal function. Dextrans were historically used to maintain circulation in shock and in the setting of reperfusion injury due to their ability to reduce endothelial cell damage from activated leukocytes. Gelatins: Gelatins are synthetic colloids composed of polypeptides produced from the degradation of bovine collagen. Gelatins are sterile, pyrogen free, do not contain preservatives, and when stored at room temperature have a 3-year expiration date. The molecular size varies, and high molecular weight products have greater oncotic effect and increased blood viscosity. However, the increase in blood volume is generally less than the amount administered due to the passage of gelatins into the interstitial space and rapid renal clearance. Similar to dextrans, gelatins also affect hemostasis by interfering with platelet function. Therefore, due to the inefficiency and potential bleeding complications, gelatins are a less commonly used colloid. Albumin infusion in patients undergoing large-volume paracentesis: A meta-analysis of randomized trials. Human albumin solution for resuscitation and volume expansion in critically ill patients. Intravenous fluids for the prevention of severe ovarian hyperstimulation syndrome. Ig preparations are concentrated, purified, filtered, and sterilized, making the risk of infectious disease transmission from Ig virtually zero. RhIg (Rh immune globulin) and other plasma derivatives are discussed in separate chapters.
¨ Gliding movements between the mandibular fossa and articular eminence occur in the upper compartment and are produced by the lateral pterygoid (protraction) and posterior fibers of the temporalis (retraction) medications you cant drink alcohol generic cytotec 200 mcg amex. Neurovasculature of infratemporal fossa: Also contained in the infratemporal fossa is the second part of the maxillary artery and its venous equivalent, the pterygoid venous plexus. The voluntary phase of the process pushes the bolus from the oral cavity into the pharynx, the expanded part of the alimentary (digestive) system, where the involuntary (automatic) phase of swallowing occurs. The size of the fissure is controlled by the peri-oral muscles, such as the orbicularis oris (the sphincter of the oral fissure), the buccinator, risorius, and depressors and elevators of the lips (dilators of the fissure). The oral cavity proper is the space between the upper and the lower dental arches or arcades (maxillary and mandibular alveolar arches and the teeth they bear). It is in the oral cavity that food and drinks are tasted and where mastication (chewing) and lingual manipulation of food occur. During chewing, the tongue (centrally), buccinator (laterally), and orbicularis oris (anteriorly) work together to retain the bolus of food between the occlusive surfaces of the molar teeth. The lips function as the valves of the oral fissure, containing the sphincter (orbicularis oris) that controls entry and exit from the mouth and upper alimentary and respiratory tracts. The labial frenula are free-edged folds of mucous membrane in the midline, extending from the vestibular gingiva to the mucosa of the upper and lower lips; the one extending to the upper lip is larger. The pulse of these arteries may be palpated by grasping the upper or lower lip lightly between the first two digits. The upper lip is supplied by superior labial branches of the facial and infra-orbital arteries. The lower lip is supplied by inferior labial branches of the facial and mental arteries. The prominence of the cheek occurs at the junction of the zygomatic and buccal regions. As the alveolar mucosa approaches the necks of the teeth, it changes in texture and color to become the gingiva proper. The alveolar mucosa (unattached gingiva) is normally shiny red and non-keratinizing. Teeth the chief functions of teeth are to: · Incise (cut), reduce, and mix food material with saliva during mastication (chewing). The gingiva proper adjacent to the tongue is the superior and inferior lingual gingivae, and that adjacent to the lips and cheeks is the maxillary and mandibular labial or buccal gingiva, respectively. The distal surface is directed away from this plane; both mesial and distal surfaces are contact surfaces-that is, surfaces that contact adjacent teeth. The root is fixed in the tooth socket by the periodontium (connective tissue surrounding roots); the number of roots varies. Pharoah, Associate Professor of Dental Radiology, Faculty of Dentistry, University of Toronto, Toronto, Ontario, Canada. The labial wall of the socket is particularly thin over the incisor teeth; the reverse is true for the molars, where the lingual wall is thinner. The periodontium (periodontal membrane) is composed of collagenous fibers that extend between the cement of the root and the periosteum of the alveolus. The cavity narrows down to the root canal in a single-rooted tooth or to one canal per root of a multirooted tooth. The root canal (pulp canal) transmits the nerves and vessels to and from the pulp cavity through the apical foramen. The incisive fossa is a depression in the midline of the bony palate posterior to the central incisor teeth into which the incisive canals open. The soft palate acts as a valve, elevating to seal the pharyngeal isthmus connecting the nasal cavity and nasopharynx with the oral cavity and oropharynx. The soft palate has no bony skeleton; however, its anterior aponeurotic part is strengthened by the palatine aponeurosis, which attaches to the posterior edge of the hard palate. When a person swallows, the soft palate initially is tensed to allow the tongue to press against it, squeezing the bolus of food to the back of the mouth. A few taste buds are located in the epithelium covering the oral surface of the soft palate, the posterior wall of the oropharynx, and the epiglottis. Each tonsil is in a tonsillar sinus (fossa), bounded by the palatoglossal and palatopharyngeal arches and the tongue. The superior lingual gingiva, the part of the gingiva covering the lingual surface of the teeth and the alveolar process, is continuous with the mucosa of the palate; therefore, injection of an anesthetic agent into the gingiva of a tooth anesthetizes the adjacent palatal mucosa. The palatine aponeurosis is formed by the merging of the flattened tendons of the right and left tensor veli palatini muscles. You can feel the transverse palatine folds and the palatine raphe with your tongue. This closes the isthmus of the pharynx, requiring that one breathes through the mouth. The orifices of the ducts of the palatine glands give the mucous membrane an orange-skin appearance. The posterior ends of the middle and inferior nasal conchae are cut through; these and the mucoperiosteum are pulled off the side wall of the nose as far as the posterior border of the medial pterygoid plate. The perpendicular plate of the palatine bone is broken through to expose the palatine nerves and arteries descending from the pterygopalatine fossa in the palatine canal. The mucosa has been removed on each side of the palatine raphe, demonstrating a branch of the greater palatine nerve on each side and the artery on the lateral side. There are four palatine arteries, two on the hard palate (greater palatine and the terminal branch of posterior nasal septal/sphenopalatine artery) and two on the soft palate (lesser palatine and ascending palatine).
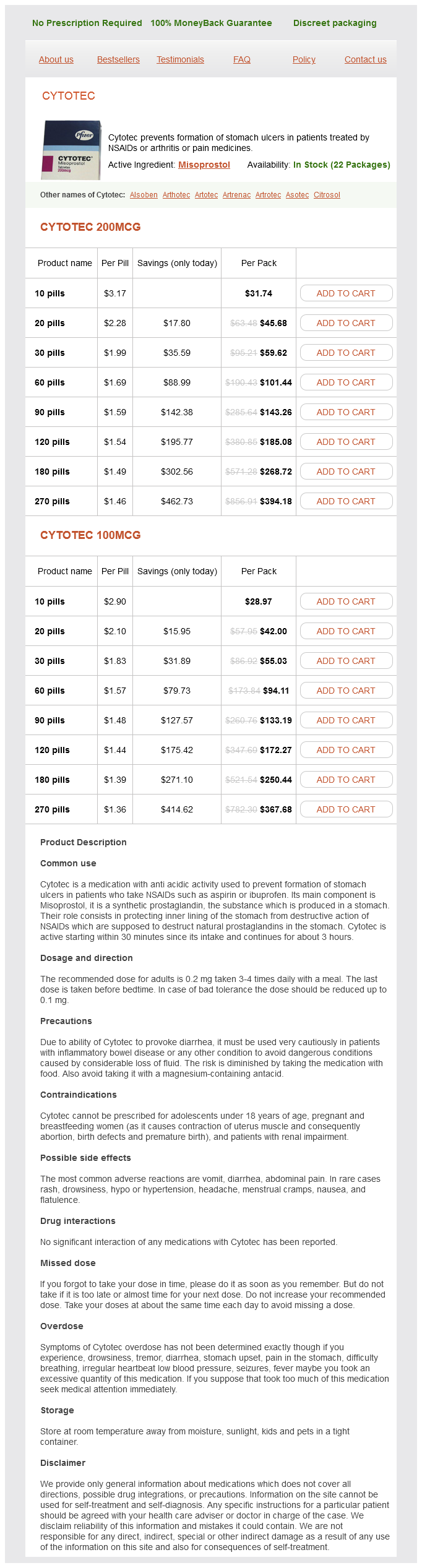
Cytotec Dosage and Price
Cytotec 200mcg
- 10 pills - $31.74
- 20 pills - $45.68
- 30 pills - $59.62
- 60 pills - $101.44
- 90 pills - $143.26
- 120 pills - $185.08
- 180 pills - $268.72
- 270 pills - $394.18
Cytotec 100mcg
- 10 pills - $28.97
- 20 pills - $42.00
- 30 pills - $55.03
- 60 pills - $94.11
- 90 pills - $133.19
- 120 pills - $172.27
- 180 pills - $250.44
- 270 pills - $367.68
Examiner applies strong internal rotation to tibia and fibula at both knee and ankle while lifting proximal fibula lanza ultimate treatment 100 mcg cytotec order otc. Knee is permitted to flex about 20; examiner then pushes medially with proximal hand and pulls with distal hand to produce a valgus force at knee. These injuries often require arthroscopically aided repair of the ligaments as necessary and repair of the injured meniscus if possible. Theplayerhearsa"pop,"feelsatearandacute pain in the knee, and may not be able to continue playing. The examiner compares the amount of play in the injured knee with that in the normal one to determine if abnormal motion is present. With the patient relaxed, the examiner attempts to slide the proximal tibia anteriorly on the femur. When As internal rotation, valgus force, and forward displacement of lateral tibial condyle are maintained, knee is passively flexed. If anterior subluxation of tibia (anterolateral instability) is present, sudden visible, audible, and palpable reduction occurs at 20 to 40 flexion. Test is positive if anterior cruciate ligament is ruptured, especially if lateral capsular ligament also is torn. At a point between 20 and 40 degrees of flexion, the iliotibial tract slides posterior to the instantaneous center of rotation of the knee and acts as a flexor, causingreductionofthetibia. Ifthe instability is a problem only during intense physical activity,usingabracemayproviderelief. Procedure same as for anterior drawer test, except that pressure on tibia is backward instead of forward. Demonstration of hyperextension Avulsion of tibial attachment, with or without small bone fragment, may be reattached with nonabsorbable sutures to firm capsular tissue or to bone or with suture through drill holes in tibia. Avulsion of femoral attachment may be repaired with nonabsorbable suture through drill holes in distal femur. The Flap formed of tendinous portion of origin of medial head of gastrocnemius muscle plus small block of bone from femoral attachment (posteromedial view). Flap passed into intercondylar notch; tunnel drilled through medial femoral condyle. With one hand fixing thigh, examiner places other hand just above ankle and applies valgus stress. If bone-to-bone repairisnot possible, manysurgeons may elect to treat the patient without resorting to surgery. Vigorousphysicaltherapy isthen institutedwhile avoidingactivities that place a load on the knee when it is flexed past 90 degrees. Complete tears, unless present with other associated injuries or in a highdemandathlete,arerarelysurgicallyrepaired. Surgical optionsincludeprimaryrepair,allograftreconstruction, and repair with anchor fixation for avulsion injuries. Injuries to this region of the knee may be associated with injuries to the popliteus tendon, iliotibial band, popliteofemoral ligament, and peroneal nerve. Posterolateral ligaments are often injured by a hyperextension mechanism, frequently with a blow to theanteromedialtibia. The external rotation recurvatum test may also be apparent on standing, giving an increased varusappearancetotheknee. On plain radiographs, a "lateral capsular sign" shows avulsion of the midportion of the lateral capsular ligament with a small fragment of proximal lateraltibia. Casesofmildinstabilitymaybe treated nonoperatively similar to that for lesser-grade sprains. Atthetimeofinjury,thepatientexperiences sudden pain, which may be associated with a tearing sensationabouttheknee. Also, the patient may not be able to maintain a passively extended knee against gravity. In both cases, surgery is required to reestablish the continuity of the quadriceps mechanism. After postoperative immobilization for 8 to 10 weeks, patients gradually start protected range-ofmotion exercises and should use a cane or walker for sometime. Circulation and nerve function must be carefully evaluated before and after reduction. Whereas apatelladislocation involves the patellofemoral joint, a knee dislocation involves the tibiofemoral articulation. Striking the knee against the dashboard during an automobile accident is the most common cause of injury, but athletic injuries are also common causes. Classification of knee dislocations is based on the position of the tibia in relation to the femur. Lateral,medial,androtational dislocations may also occur, as may combination patterns such as anterolateral and posterolateral. Tear or thrombosis of popliteal artery is a frequent complication, requiring immediate repair or replacement. Tibial and common peroneal nerves may also be torn but usually do not require surgical repair. Four-compartment fasciotomy must be done at the first sign of compartment syndrome.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.