
Dapagliflozin
General Information about Dapagliflozin
In conclusion, dapagliflozin, or Forxiga, is an efficient and protected possibility for the administration of type 2 diabetes. Its distinctive mechanism of motion and potential additional benefits make it a valuable addition to the prevailing arsenal of diabetes drugs. However, it is essential to keep in thoughts that dapagliflozin isn't a cure for type 2 diabetes, and it ought to be used as part of a complete remedy plan that options a healthy diet and regular train. With correct use and monitoring, dapagliflozin can help folks with sort 2 diabetes obtain higher glycemic control and enhance their overall well being and well-being.
In addition to its glucose-lowering effects, dapagliflozin has been found to have other potential benefits for people with type 2 diabetes. Research suggests that it might help to enhance coronary heart and kidney health by lowering the chance of cardiovascular occasions and delaying the progression of diabetic kidney illness. These benefits are especially vital because people with kind 2 diabetes are at the next threat of creating cardiovascular problems and kidney disease.
Dapagliflozin belongs to a category of medicines referred to as sodium-glucose cotransporter 2 (SGLT2) inhibitors. It works by blocking the absorption of glucose within the kidneys, leading to elevated excretion of glucose within the urine. This mechanism of action is different from other diabetes medications, which primarily work by increasing insulin manufacturing or bettering insulin sensitivity. By lowering the quantity of glucose in the bloodstream, dapagliflozin helps to cut back blood sugar levels and improves glycemic management in people with sort 2 diabetes.
As with any medication, dapagliflozin might cause some unwanted effects. These include urinary tract infections, yeast infections, and increased frequency of urination. It is crucial to discuss any potential unwanted effects with a healthcare skilled and report any regarding signs promptly. Additionally, dapagliflozin might interact with different drugs, and it's essential to inform a well being care provider of all current medicines earlier than starting remedy.
Clinical trials have shown dapagliflozin to be effective in reducing HbA1c ranges, a long-term measure of blood sugar control, and in bettering other glycemic parameters similar to fasting and postprandial blood sugar levels. It has also been discovered to be helpful in decreasing weight and body mass index (BMI) in people with sort 2 diabetes. This is particularly necessary as a result of obesity is a major danger issue for creating the condition and might make glucose management more difficult. Moreover, dapagliflozin has been proven to have a favorable safety profile, with minimal threat of hypoglycemia (low blood sugar levels) in comparison with other diabetes medications.
Dapagliflozin, commonly known by its model name Forxiga, is a medication used for the administration of sort 2 diabetes. In recent years, the prevalence of sort 2 diabetes has been on the rise, making it a global well being concern. As the variety of individuals living with this condition continues to increase, the necessity for effective remedies turns into extra obvious. Dapagliflozin has emerged as a promising medicine in the struggle towards sort 2 diabetes and is gaining popularity among healthcare professionals and patients alike.
Forxiga is a prescription medicine and must be used under the steering of a healthcare professional. It is out there in tablet kind and is often taken as soon as a day, with or with out meals. The recommended dosage may range based on particular person needs, and it is important to follow the physician's instructions carefully. The medicine shouldn't be crushed or chewed, but swallowed whole with a glass of water.
It receives sensory information through spinal lipoatrophy definition diabetes generic dapagliflozin 10 mg on line, trigeminal and vestibulocerebellar pathways and, via the pontine nuclei, from the cerebral cortex and the tectum. Cerebellar output is mainly to those structures of the brain that control movement. The basic internal organization of the cerebellum is that of a superficial, highly convoluted cortex (a laminated sheet of neurones and supporting cells) overlying a dense core of white matter. The latter contains deep cerebellar nuclei, which give rise to the efferent cerebellar projections. Although the human cerebellum makes up approximately one-tenth of the entire brain by weight, the surface area of the cerebellar cortex, if unfolded, would be about half that of the cerebral cortex. The great majority of cerebellar neurones are small granule cells; they are so densely packed that the cerebellar cortex contains many more neurones than the cerebral cortex. Unlike the cerebral cortex, where a large number of diverse cell types are arranged differently in different regions, the cerebellar cortex contains a relatively small number of different cell types that are interconnected in a highly stereotypical way. Disease processes affecting the cerebellum or its connections lead to incoordination. Movements of the eyes, speech apparatus, individual limbs and balance are usually affected, which results in nystagmus, dysarthria, incoordination and ataxia. Although all these movements become defective in widespread disease of the cerebellum or its connections, topographical arrangements within the cerebellum lead to a variety of clinically recognizable disease patterns. Thus, in cerebellar hemisphere disease, the ipsilateral limbs show rhythmical tremor during movement but not at rest. The tremor increases as the target is approached, so reaching and accurate movements of the arm are especially difficult. Diseases that affect the ascending spinocerebellar pathways or the midline vermis have a disproportionate effect on axial structures, leading to severe loss of balance. Lesions of outflow tracts in the superior cerebellar peduncles result in a wide-amplitude, severely disabling, proximal tremor that interferes with all movements and may even disturb posture, leading to rhythmic oscillations of the head or trunk so that the patient is unable to stand or sit without support. However, although cerebellar lesions may initially cause profound motor impairment, a considerable degree of recovery is possible. There are clinical reports that the initial symptoms of large cerebellar lesions (caused by trauma or surgical excision) have improved progressively over time. Although the basic structure of the cerebellum and its importance for normal movement have long been recognized, many of the details of how it functions remain obscure. The main goal of this chapter is to describe the known structure and connections of the cerebellum. The transverse sinus borders the cerebellum at the point where the superior and inferior surfaces meet. The inferior surface is characterized by a massive enlargement of the cerebellar hemispheres, which extends medially to overlie some of the vermis. Posteriorly, the hemispheres are separated by a deep vallecula, which contains the dural falx cerebelli. It forms the roof of the fourth ventricle and the lateral recesses on each side of it, while the cerebellar peduncles define the diamond shape of the ventricle when viewed from behind. Anterolaterally, the cerebellum lies against the posterior surface of the petrous part of the temporal bone. The cerebellar surface is divided by numerous curved transverse fissures that separate its folia and give it a laminated appearance. One conspicuous fissure, the horizontal fissure, extends around the dorsolateral border of each hemisphere from the middle cerebellar peduncle to the vallecula, separating the superior and inferior surfaces. Although the horizontal fissure is prominent, it appears relatively late in embryological development and does not mark the boundary between major functional subdivisions of the cortex. The deepest fissure in the vermis is the primary fissure, which curves ventrolaterally around the superior surface of the cerebellum to meet the horizontal fissures. It appears early in embryological development and marks the boundary between the anterior and posterior lobes. Because the cerebellar cortex has a roughly spherical shape, the true relations between its parts can sometimes be obscured. Thus, the most anterior lobule of the cerebellar vermis, the lingula, lies very close to the most posterior lobule, the nodule. The lobules of the superior vermis that belong to the anterior lobe are the lingula, central lobule and culmen. The central lobule and culmen are continuous bilaterally with an adjoining wing (ala) in each hemisphere. The culmen (with attached anterior quadrangular lobules) lies between the preculminary and primary fissures. Between the primary and horizontal fissures are the simple lobule (with attached posterior quadrangular lobules) and the folium (with attached superior semilunar lobules). From the back forward, the inferior vermis is divided into the tuber, pyramis, uvula and nodule, in that order. The tuber is continuous laterally with the inferior semilunar lobules and separated from the pyramis by the lunogracile fissure. The pyramis and attached biventral lobules (containing an intrabiventral fissure) are separated from the uvula and attached cerebellar tonsils by the secondary fissure. Behind the uvula, and separated from it by the median part of the posterolateral fissure, is the nodule. The tonsils are roughly spherical and overhang the foramen magnum on each side of the medulla oblongata.
Remember diabetes diet holistic dapagliflozin 10 mg order otc, all the other cranial nerves may rarely be affected owing to overgrowth of foramina or basilar invagination, so examine them carefully. These patients have a short neck and low hairline, the head is held in extension and neck movements are decreased. Assess the jugular venous pressure and examine the heart for signs of cardiac failure due to a hyperdynamic circulation. Look at the legs for anterior bowing of the tibia and lateral bowing of the femur. There may be limitation of hip movements especially abduction, which suggests protrusio acetabuae and fixed flexion deformity of the knees. Sarcomas (a feared, but rare, complication) should be looked for, particularly in the femur, humerus and skull; they usually present as tender, localised swellings. The serum alkaline phosphatase level is an indicator of disease activity, as is the urinary hydroxyproline level. Look for bony enlargement, increased density, an irregular widened cortex and cortical infractions (incomplete pseudofractures) on the convex side of the bowed long bones. The early lytic phase of the disease, presenting with a flame-shaped osteolytic wedge advancing along the bones, is often overlooked. Bone scanning is more sensitive l-m ed ic in e- vi de os 10 · the endocrine long case 275 than an X-ray in assessing the extent of disease. Treatment the indications for treatment are bone pain, progressive deformity or complications such as neural compression or high-output cardiac failure, and as a prelude to orthopaedic surgery. Treatment of patients with Pagetic involvement of weight-bearing bones may be indicated to attempt to prevent deformity and pathological fracture. These drugs are effective at reducing hydroxyproline excretion and often relieve symptoms, but may exacerbate bone pain initially. However, bone turnover is reduced and new bone is usually more normal in structure. The bisphosphonates should be given in combination with calcium supplements and vitamin D. Intravenous infusions of the potent bisphosphonate pamidronate may produce prolonged suppression of Pagetic activity and may normalise bone turnover in patients with mild disease without adverse effects on bone mineralisation or bone formation. Calcitonin of salmon or human origin, given subcutaneously, often improves bone pain and may be useful in the treatment of neurological complications. Although side-effects (nausea, flushing and diarrhoea) are common and may limit treatment in up to 20% of patients, it is still second-line therapy. Resistance to salmon calcitonin after 12 years may indicate the development of neutralising antibodies. Serum alkaline phosphatase levels and urinary hydroxyproline levels are useful guides to the effect of treatment; a 50% reduction in either test value indicates a good response to treatment. There may be significant increases in bone lysis and predisposition to fractures with this drug, as well as bone marrow depression. It is important for the patient to avoid immobilisation in the postoperative period because of the risk of hypercalcaemia. Preoperative chemotherapy followed by amputation the current treatment for spontaneously occurring tumours is being evaluated. There is also an increase in the incidence of colonic polyps and carcinoma of the colon. There is now a recognised association with obstructive sleep apnoea and questions should be asked about snoring, daytime sleepiness and other relevant symptoms. The reason for the association is the enlargement of the tongue and swelling of the upper airway. Ask if the patient knows what investigations have been performed (see investigations below). The patient may be in hospital for these tests because of a complication of the condition or, perhaps more likely, has been brought in for the clinical examinations. Find out when the diagnosis was made and how long ago; in retrospect, the patient may have had symptoms for years. Ask what changes the patient has been aware of and whether these have improved with treatment. Failure of suppression is characteristic of acromegaly, but the test is non-specific and may be abnormal in renal impairment, thyrotoxicosis and diabetes. In 25% of acromegalic patients, the prolactin level is elevated and this can be associated with galactorrhoea. Other pituitary hormone levels may be low because of interference with normal pituitary function by the large mass of the tumour. If the tumour is close to the optic chiasm then visual field assessment should be performed. Investigate for complications: · HbA1c · sleep study · echocardiogram · colonoscopy. Medical treatment with long-acting somatostatin analogues is increasingly useful, both before surgery and afterwards if removal is incomplete. Selective resection of the benign adenoma and preservation pituitary function is possible in 5080% of surgically treated cases. Nevertheless, symptoms are almost always greatly relieved by surgical debulking of the tumour. Uncommon complications include cerebrospinal fluid rhinorrhoea, diabetes insipidus and stroke. Gastrointestinal: colonoscopy for polyps at diagnosis and as required for surveillance.
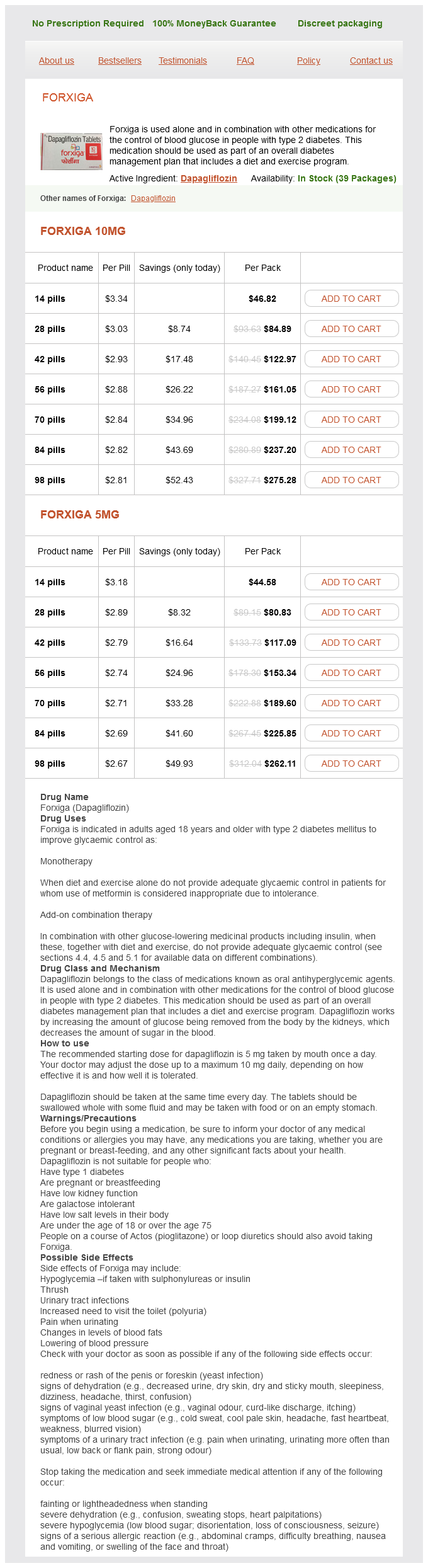
Dapagliflozin Dosage and Price
Forxiga 10mg
- 14 pills - $46.82
- 28 pills - $84.89
- 42 pills - $122.97
- 56 pills - $161.05
- 70 pills - $199.12
- 84 pills - $237.20
- 98 pills - $275.28
Forxiga 5mg
- 14 pills - $44.58
- 28 pills - $80.83
- 42 pills - $117.09
- 56 pills - $153.34
- 70 pills - $189.60
- 84 pills - $225.85
- 98 pills - $262.11
It contains narrow longitudinal bundles of fibres on each side blood glucose 60 proven 10 mg dapagliflozin, the medial and lateral longitudinal striae. Posteriorly, the indusium griseum is continuous with the dentate gyrus and hippocampus through the gyrus fasciolaris. The splenium of the corpus callosum overhangs the posterior ends of the thalami, the pineal gland and the tectum but is separated from them by several structures. On each side, the crus of the fornix and gyrus fasciolaris curve up to the splenium. The crus continues forward on the inferior surface of the callosal trunk, but the gyrus fasciolaris skirts above the splenium, then rapidly diminishes into the indusium griseum. The tela choroidea of the third ventricle advances below the splenium through the transverse fissure, and the internal cerebral veins emerge between its two layers to form the great cerebral vein. Posteriorly, the splenium is near the tentorium cerebelli, great cerebral vein and beginning of the straight sinus. Nerve fibres of the corpus callosum radiate into the white matter core of each hemisphere, thereafter dispersing to the cerebral cortex. Commissural fibres forming the rostrum extend laterally, below the anterior horn of the lateral ventricle, connecting the orbital surfaces of the frontal lobes. Fibres in the genu curve forward, as the forceps minor, to connect the lateral and medial surfaces of the frontal lobes. Fibres of the trunk and splenium, which form the roof and lateral wall of the posterior horn and the lateral wall of the inferior horn of the lateral ventricle, constitute the tapetum. The remaining fibres of the splenium curve back into the occipital lobes as the forceps major. Not all interhemispheric connections through the corpus callosum represent a simple linking of loci in one hemisphere with the same loci in the other. This is seen most clearly for the visual areas, where the cortex containing the representation of each midline retinal zone is linked to its counterpart on the contralateral side. A similar arrangement is seen in somatic areas, where the trunk representation is callosally linked, but the peripheral limb areas (hands and feet) are not. Connections that link the same or similar areas on each side are termed homotopic connections. The corpus callosum also interconnects heterogeneous cortical areas on the two sides (heterotopic connections). These may serve to connect functionally similar but anatomically different loci in the two hemispheres or to connect functional areas in one hemisphere with regions that are specialized for a unilaterally confined function in the other. This is perhaps not surprising, because apparently little disturbance of function occurs when large parts, and in some cases all, of the corpus callosum are surgically divided for the control of intractable epilepsy. The anterior commissure is a compact bundle of myelinated nerve fibres that crosses anterior to the columns of the fornix and is embedded in the lamina terminalis, where it is part of the anterior wall of the third ventricle. The smaller anterior bundle curves forward on each side to the anterior perforated substance and olfactory tract. The posterior bundle curves posterolaterally on each side in a deep groove on the anteroinferior aspect of the lentiform complex and subsequently fans out into the anterior part of the temporal lobe, including the parahippocampal gyrus. Areas thought to be connected via commissural fibres include the olfactory bulb and anterior olfactory nucleus; the anterior perforated substance, olfactory tubercle and diagonal band of Broca; the prepiriform cortex; the entorhinal area and adjacent parts of the parahippocampal gyrus; part of the amygdaloid complex, especially the nucleus of the lateral olfactory stria; the bed nucleus of the stria terminalis and the nucleus accumbens; and the anterior regions of the middle and inferior temporal gyri. Projection fibres connect the cerebral cortex with lower levels in the brain and spinal cord. Corticofugal projection fibres converge from all directions to form the dense subcortical white matter mass of the corona radiata. Large numbers of fibres pass to the corpus striatum and the thalamus, intersecting commissural fibres of the corpus callosum en route. The corona radiata is continuous with the internal capsule, which contains the majority of the cortical projection fibres. Anterior Commissure Projection Fibres 306 Chapter 16 / Cerebral Hemispheres Posterior limb of internal capsule Corona radiata Anterior limb of internal capsule. It has an anterior limb, genu, posterior limb, and retrolenticular (retrolentiform) and sublenticular (sublentiform) parts. The head of the caudate nucleus is medial to the anterior limb, and the thalamus is medial to the posterior limb. Cortical efferent fibres of the internal capsule continue to converge as they descend. Fibres derived from the frontal lobe tend to pass posteromedially, whereas temporal and occipital fibres pass anterolaterally. Many, but not all, corticofugal fibres pass into the crus cerebri of the ventral midbrain. There, corticospinal and corticobulbar fibres are located in the middle half of the crus. Frontopontine fibres are located medially, whereas corticopontine fibres from temporal, parietal and occipital cortices are found laterally. The anterior limb of the internal capsule contains frontopontine fibres, which arise from the cortex in the frontal lobe. Axons of these cells enter the opposite cerebellar hemisphere through the middle cerebellar peduncle. Anterior thalamic radiations interconnect the medial and anterior thalamic nuclei and various hypothalamic nuclei and limbic structures with the frontal cortex.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.