
Dipyridamole
General Information about Dipyridamole
In conclusion, dipyridamole is an important treatment within the prognosis and remedy of coronary artery illness. It allows for accurate evaluation of the heart's blood circulate in sufferers who're unable to exercise sufficiently, offering priceless info for correct management of the situation. As with any treatment, it's essential to comply with the prescribed dosage and report any opposed reactions to a healthcare supplier.
Dipyridamole can also be used in mixture with other medicines for the remedy of angina, a kind of chest pain that occurs when the guts does not receive sufficient blood and oxygen. This medicine might help alleviate symptoms of angina by rising blood circulate to the center.
Like any medicine, dipyridamole could trigger unwanted effects in some people. Common unwanted facet effects embrace headache, dizziness, nausea, and abdomen upset. More serious unwanted side effects corresponding to problem respiration or modifications in heart rate must be reported to a healthcare supplier instantly.
Thallium imaging, also referred to as a cardiac blood move scan, is a diagnostic take a look at that uses a radioactive substance to judge the blood flow to the center. This take a look at is typically carried out after exercise, as bodily exercise can increase heart fee and blood circulate, making it simpler to detect any abnormalities. However, not all sufferers are capable of train adequately because of varied medical reasons similar to age, disability, or different health situations. In these circumstances, dipyridamole is used to simulate the effects of exercise on the center.
Dipyridamole works by dilating the blood vessels in the body, including these of the guts. This dilation increases the blood move to the center, mimicking the results of exercise. As a result, the thallium imaging check can precisely assess the blood move to the heart, providing valuable data on any potential blockages.
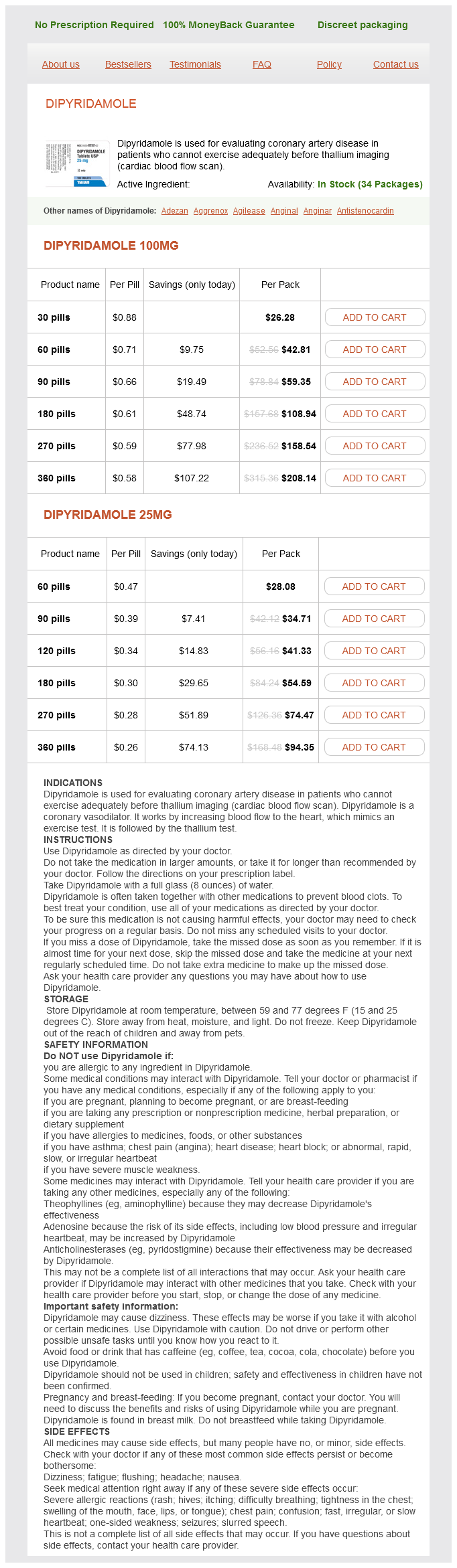
Dipyridamole is a medication that's generally used in the analysis of coronary artery disease in patients who usually are not able to train sufficiently earlier than a thallium imaging take a look at. This medicine works by rising the blood circulate to the center, allowing for a extra correct assessment of the guts's operate and potential blockages within the coronary arteries.
To carry out the thallium imaging take a look at with dipyridamole, the patient is given an oral dose of the medication, normally within the form of a tablet. The affected person is then instructed to relaxation for a brief period, after which the radioactive thallium is given intravenously. The affected person is monitored for any opposed reactions through the test.
Coronary artery illness is a situation by which the arteries that supply blood to the guts turn into narrowed or blocked, resulting in a lower in blood flow to the heart. This may find yourself in chest pain, shortness of breath, and in severe circumstances, heart assault. Timely and accurate analysis of coronary artery illness is crucial for correct therapy and administration of the situation.
In contrast hypertension canada discount dipyridamole online mastercard, benzodiazepines and the newer hypnotics do not change hepatic drugmetabolizing enzyme activity with continuous use. Multiple subunits of several of these classes have been characterized, eg, six different, four, and three. Strains of mice, in which a point mutation has been inserted converting histidine to arginine in the 1 subunit, show resistance to both the sedative and amnestic effects of benzodiazepines, but anxiolytic and muscle-relaxing effects are largely unchanged. Other mutation studies have led to suggestions that an 5 subtype is involved in at least some of the memory impairment caused by benzodiazepines. A hetero-oligomeric glycoprotein, the complex consists of five or more membrane-spanning subunits. Binding of benzodiazepines and the newer hypnotic drugs such as zolpidem occurs at a single site between and subunits, facilitating the process of chloride ion channel opening. The benzodiazepine antagonist flumazenil also binds at this site and can reverse the hypnotic effects of zolpidem. These effects involve a binding site or sites distinct from the benzodiazepine binding sites. This multiplicity of sites of action of barbiturates may be the basis for their ability to induce full surgical anesthesia (see Chapter 25) and for their more pronounced central depressant effects (which result in their low margin of safety) compared with benzodiazepines and the newer hypnotics. In addition to the benzodiazepines, barbiturates, and the newer hypnotics (eg, zolpidem), many other drugs with central nervous system effects can modify the function of this important ionotropic receptor. These include alcohol and certain intravenous anesthetics (etomidate, propofol) in addition to thiopental. However, it has not been shown that all these drugs act exclusively by this mechanism. Central nervous system excitatory agents that act on the chloride channel include picrotoxin and bicuculline. Hypnosis-By definition, all of the sedative-hypnotics induce sleep if high enough doses are given. The effects of sedativehypnotics on the stages of sleep depend on several factors, including the specific drug, the dose, and the frequency of its administration. More rapid onset of sleep and prolongation of stage 2 are presumably clinically useful effects. However, rebound insomnia occurs with both zolpidem and zaleplon if used at higher doses. Despite possible reductions in slow-wave sleep, there are no reports of disturbances in the secretion of pituitary or adrenal hormones when either barbiturates or benzodiazepines are used as hypnotics. The use of sedative-hypnotics for more than 12 weeks leads to some tolerance to their effects on sleep patterns. However, the suitability of a particular agent as an adjunct in anesthesia depends mainly on the physicochemical properties that determine its rapidity of onset and duration of effect. Among the barbiturates, thiopental and methohexital are very lipid-soluble, penetrating brain tissue rapidly following intravenous administration, a characteristic favoring their use for the induction of anesthesia. Rapid tissue redistribution (not rapid elimination) accounts for the short duration of action of these drugs, a feature useful in recovery from anesthesia. In addition to their direct actions, these molecules can block the effects of benzodiazepines. Sedation-Benzodiazepines, barbiturates, and most older sedative-hypnotic drugs exert calming effects with concomitant reduction of anxiety at relatively low doses. In most cases, however, the anxiolytic actions of sedative-hypnotics are accompanied by some depressant effects on psychomotor and cognitive functions. In experimental animal models, benzodiazepines and older sedativehypnotic drugs are able to disinhibit punishment-suppressed behavior. This disinhibition has been equated with antianxiety effects of sedative-hypnotics, and it is not a characteristic of all drugs that have sedative effects, eg, the tricyclic antidepressants and antihistamines. Not surprisingly, benzodiazepines given in large doses as adjuncts to general anesthetics may contribute to a persistent postanesthetic respiratory depression. This is probably related to their relatively long half-lives and the formation of active metabolites. However, such depressant actions of the benzodiazepines are usually reversible with flumazenil. Several benzodiazepines-including clonazepam, nitrazepam, lorazepam, and diazepam-are sufficiently selective to be clinically useful in the management of seizures (see Chapter 24). Of the barbiturates, phenobarbital and metharbital (converted to phenobarbital in the body) are effective in the treatment of generalized tonic-clonic seizures, though not the drugs of first choice. Muscle relaxation-Certain drugs in the sedative-hypnotic class, particularly members of the carbamate (eg, meprobamate) and benzodiazepine groups, exert inhibitory effects on polysynaptic reflexes and internuncial transmission and at high doses may also depress transmission at the skeletal neuromuscular junction. Somewhat selective actions of this type that lead to muscle relaxation can be readily demonstrated in animals and have led to claims of usefulness for relaxing contracted voluntary muscle in muscle spasm (see Clinical Pharmacology of Sedative-Hypnotics). Muscle relaxation is not a characteristic action of zolpidem, zaleplon, and eszopiclone. Effects on respiration and cardiovascular function- At hypnotic doses in healthy patients, the effects of sedativehypnotics on respiration are comparable to changes during natural sleep. However, even at therapeutic doses, sedative-hypnotics can produce significant respiratory depression in patients with pulmonary disease. Effects on respiration are dose-related, and depression of the medullary respiratory center is the usual cause of death due to overdose of sedative-hypnotics. At doses up to those causing hypnosis, no significant effects on the cardiovascular system are observed in healthy patients. However, in hypovolemic states, heart failure, and other diseases that impair cardiovascular function, normal doses of sedativehypnotics may cause cardiovascular depression, probably as a result of actions on the medullary vasomotor centers. At toxic doses, myocardial contractility and vascular tone may both be depressed by central and peripheral effects, possibly via facilitation of the actions of adenosine, leading to circulatory collapse.
Amiodarone has unusual pharmacokinetics and important extracardiac adverse effects blood pressure medication and q10 cheap 25 mg dipyridamole otc. Celivarone is another noniodinated benzofuran derivative similar to dronedarone that is currently undergoing clinical trials for the prevention of ventricular tachycardia recurrence. It is a relatively potent sodium channel blocker that does not prolong action potential duration. As described in Chapter 10, some of these drugs have selectivity for cardiac 1 receptors, some have intrinsic sympathomimetic activity, some have marked direct membrane effects, and some prolong the cardiac action potential. The relative contributions of the -blocking and direct membrane effects to the antiarrhythmic effects of these drugs are not fully known. Although blockers are fairly well tolerated, their efficacy for suppression of ventricular ectopic depolarizations is lower than that of sodium channel blockers. However, there is good evidence that these agents can prevent recurrent infarction and sudden death in patients recovering from acute myocardial infarction (see Chapter 10). Esmolol is a short-acting blocker used primarily as an antiarrhythmic drug for intraoperative and other acute arrhythmias. Sotalol is a nonselective -blocking drug that prolongs the action potential (class 3 action). The action potential duration is prolonged uniformly over a wide range of heart rates; that is, the drug does not have reverse use-dependent action. Despite its present classification as a class 3 agent, amiodarone also significantly blocks inactivated sodium channels. Action potential prolongation by most of these drugs exhibits the undesirable property of "reverse use-dependence": action potential prolongation is least marked at fast rates (where it is desirable) and most marked at slow rates, where it can contribute to the risk of torsades de pointes. This action is prominent after intravenous administration and may be related to the action of the vehicle. The drug accumulates in many tissues, including the heart (1050 times more so than in plasma), lung, liver, and skin, and is concentrated in tears. Abnormal liver function tests and hypersensitivity hepatitis may develop during amiodarone treatment and liver function tests should be monitored regularly. The skin deposits result in a photodermatitis and a gray-blue skin discoloration in sun-exposed areas, eg, the malar regions. After a few weeks of treatment, asymptomatic corneal microdeposits are present in virtually all patients treated with amiodarone. Amiodarone blocks the peripheral conversion of thyroxine (T4) to triiodothyronine (T3). Thyroid function should be evaluated before initiating treatment and should be monitored periodically. Because effects have been described in virtually every organ system, amiodarone treatment should be reevaluated whenever new symptoms develop in a patient, including arrhythmia aggravation. The drug increases the pacing and defibrillation threshold, and these devices require retesting after a maintenance dose has been achieved. The design was intended to eliminate action of the parent drug on thyroxine metabolism and to modify the half-life of the drug. No thyroid dysfunction or pulmonary toxicity has been reported in short-term studies. However, liver toxicity, including two severe cases requiring liver transplantation, has been reported. The drug has a half-life of 24 hours and can be administered twice daily at a fixed dose of 400 mg. Dronedarone absorption increases twofold to threefold when taken with food, and this information should be communicated to patients as a part of the dosing instructions. It inhibits tubular secretion of creatinine, resulting in a 1020% increase in serum creatinine; however, because the glomerular filtration rate is unchanged, no adjustments are required. Dronedarone restores sinus rhythm in a small percentage of patients (< 15%) with atrial fibrillation. It produces a 10- to 15-bpm reduction of the ventricular rate compared to placebo. In one report, dronedarone doubled the interval between episodes of atrial fibrillation recurrence in patients with paroxysmal atrial fibrillation. Initial studies suggested a reduction in mortality or hospitalization in patients with atrial fibrillation. Similarly, a trial of dronedarone in advanced heart failure was terminated prematurely because of an increase in mortality. Pharmacokinetics Amiodarone is variably absorbed with a bioavailability of 3565%. It undergoes hepatic metabolism, and the major metabolite, desethylamiodarone, is bioactive. The elimination half-life is complex, with a rapid component of 310 days (50% of the drug) and a slower component of several weeks. Amiodarone has many important drug interactions, and all medications should be reviewed when the drug is initiated and when the dose is adjusted. Amiodarone inhibits several cytochrome P450 enzymes and may result in high levels of many drugs, including statins, digoxin, and warfarin. The dose of warfarin should be reduced by one third to one half following initiation of amiodarone, and prothrombin times should be closely monitored. All the -adrenergic-blocking activity resides in the l-isomer; the d- and l-isomers share action potential prolonging effects. Beta-adrenergic-blocking action is not cardioselective and is maximal at doses below those required for action potential prolongation. It is not associated with an increase in mortality in patients with coronary artery disease or heart failure.
Dipyridamole Dosage and Price
Dipyridamole 100mg
- 30 pills - $26.28
- 60 pills - $42.81
- 90 pills - $59.35
- 180 pills - $108.94
- 270 pills - $158.54
- 360 pills - $208.14
Dipyridamole 25mg
- 60 pills - $28.08
- 90 pills - $34.71
- 120 pills - $41.33
- 180 pills - $54.59
- 270 pills - $74.47
- 360 pills - $94.35
Adrenoreceptors were initially characterized pharmacologically by their relative affinities for agonists; receptors have the comparative potencies epinephrine norepinephrine >> isoproterenol blood pressure chart bpm order dipyridamole 100 mg with amex, and receptors have the comparative potencies isoproterenol > epinephrine norepinephrine. The presence of subtypes of these receptors were further characterized by molecular cloning. Stimulation of 1 receptors by catecholamines leads to the activation of a Gq-coupling protein. Ca2+ may then activate Ca2+-dependent protein kinases, which in turn phosphorylate their substrates. These receptors are particularly important in the brain (see Chapters 21, 28, and 29) and in the splanchnic and renal vasculature. Molecular cloning has identified several distinct genes encoding five receptor subtypes, two D1-like receptors (D1 and D5) and three D2-like receptors (D2, D3, and D4). Further complexity occurs because of the presence of introns within the coding region of the D2-like receptor genes, which allows for alternative splicing of the exons in this major subtype. These subtypes may have importance for understanding the efficacy and adverse effects of novel antipsychotic drugs (see Chapter 29). Alpha Receptors Alpha1 receptors are coupled via G proteins in the Gq family to phospholipase C. In addition, 1 receptors activate signal transduction pathways that stimulate tyrosine kinases. It is likely that not only, but also the - subunits of Gi contribute to inhibition of adenylyl cyclase. Alpha2 receptors use other signaling pathways, including regulation of ion channel activities and the activities of important enzymes involved in signal transduction. Activation of the cyclase enzyme is mediated by the stimulatory coupling protein Gs. The 3 adrenoreceptor is a lower affinity receptor compared with 1 and 2 receptors but is more resistant to desensitization. It is found in several tissues, but its physiologic or pathologic role in humans is not clear. Mirabegron, a selective 3 agonist, is approved for the treatment of symptoms of overactive bladder (urinary urgency and frequency). A small increase in blood pressure was observed in clinical trials; the longterm significance of this finding is not clear. D2 receptors have been found to inhibit adenylyl cyclase activity, open potassium channels, and decrease calcium influx. Relative Receptor Affinities Alpha agonists Phenylephrine, methoxamine Clonidine, methylnorepinephrine Mixed alpha and beta agonists Norepinephrine Epinephrine Beta agonists Dobutamine1 Isoproterenol Albuterol, terbutaline, metaproterenol, ritodrine Dopamine agonists Dopamine Fenoldopam 1 1 > 2 >>>>> 2 > 1 >>>>> 1 = 2; 1 >> 2 1 = 2; 1 = 2 1 > 2 >>>> 1 = 2 >>>> 2 >> 1 >>>> D1 = D2 >> >> D1 >> D2 See text. Receptor Selectivity Examples of clinically useful sympathomimetic agonists that are relatively selective for 1-, 2-, and -adrenoceptor subgroups are compared with some nonselective agents in Table 92. Selectivity means that a drug may preferentially bind to one subgroup of receptors at concentrations too low to interact extensively with another subgroup. However, selectivity is not usually absolute (nearly absolute selectivity has been termed "specificity"), and at higher concentrations, a drug may also interact with related classes of receptors. The effects of a given drug may depend not only on its selectivity to adrenoreceptor types, but also to the relative expression of receptor subtypes in a given tissue. The magnitude of the response depends on the number and function of adrenoceptors on the cell surface and on the regulation of these receptors by catecholamines themselves, other hormones and drugs, age, and a number of disease states (see Chapter 2). One of the best-studied examples of receptor regulation is the desensitization of adrenoceptors that may occur after exposure to catecholamines and other sympathomimetic drugs. Other terms such as tolerance, refractoriness, and tachyphylaxis have also been used to denote desensitization. This process has potential clinical significance because it may limit the therapeutic response to sympathomimetic agents. Some mechanisms occur relatively slowly, over the course of hours or days, and these typically involve transcriptional or translational changes in the receptor protein level, or its migration to the cell surface. Rapid modulation of receptor function in desensitized cells may involve critical covalent modification of the receptor, especially by phosphorylation of specific amino acid residues, association of these receptors with other proteins, or changes in their subcellular location. There are two major categories of desensitization of responses mediated by G protein-coupled receptors. Homologous desensitization refers to loss of responsiveness exclusively of the receptors that have been exposed to repeated or sustained activation by an agonist. Heterologous desensitization refers to the process by which desensitization of one receptor by its agonists also results in desensitization of another receptor that has not been directly activated by the agonist in question. Specific adrenoceptors become substrates for these kinases only when they are bound to an agonist. This mechanism is an example of homologous desensitization because it specifically involves only agonist-occupied receptors. Phosphorylation of these receptors enhances their affinity for arrestins, a family of four proteins, of which the two nonvisual arrestin subtypes are widely expressed. In addition to desensitizing agonist responses mediated by G proteins, arrestins can trigger G protein-independent signaling pathways. Recognition that G protein-coupled receptors can signal through both G protein-coupled and G protein-independent pathways has raised the concept of developing biased agonists that selectively activate these arrestin-coupled signaling pathways (see Box: Therapeutic Potential of Biased Agonists at Beta Receptors). For the 2 receptor, protein kinase A phosphorylation occurs on serine residues in the third cytoplasmic loop of the receptor. Similarly, activation of protein kinase C by Gq-coupled receptors may lead to phosphorylation of this class of G protein-coupled receptors. This second-messenger feedback mechanism has been termed heterologous desensitization because activated protein kinase A or protein kinase C may phosphorylate any structurally similar receptor with the appropriate consensus sites for phosphorylation by these enzymes. Beta1 receptors are also coupled through G protein-independent signaling pathways involving -arrestin, which are thought to be cardioprotective.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.