
Evista
General Information about Evista
In addition to preventing bone loss and lowering the chance of breast cancer, Evista additionally has some other potential advantages. It has been shown to enhance general bone health, reduce the danger of vertebral fractures, and improve levels of cholesterol. It may also have a constructive effect on cardiovascular health, as postmenopausal ladies are at an elevated risk for heart illness.
Osteoporosis is a condition that impacts hundreds of thousands of ladies around the world. This bone illness weakens the bones, making them extra vulnerable to fractures and breaks. It is mostly seen in postmenopausal women due to the decreased levels of estrogen, a hormone that helps maintain bone density. While there are various therapy options out there, one medication that has gained reputation in current times is Evista.
In conclusion, Evista is a extensively used and effective medicine for the treatment of postmenopausal osteoporosis. Not only does it assist to prevent bone loss and enhance bone density, however it additionally has the additional advantage of reducing the danger of invasive breast most cancers. However, like all medicine, it could be very important weigh the potential benefits and risks and to have common check-ups with a doctor whereas taking Evista. With proper use and monitoring, Evista can be a useful device in the fight in opposition to osteoporosis and breast most cancers in postmenopausal women.
While Evista might sound like a miracle drug, you will need to notice that it is not appropriate for everybody. It is just really helpful for postmenopausal women with osteoporosis, as it is not efficient in preventing bone loss in premenopausal girls or in men. It can be not recommended for use in women who're pregnant or breastfeeding, as nicely as those with a history of blood clots or stroke.
Evista is an oral medication that belongs to a class of medicine referred to as selective estrogen receptor modulators (SERMs). It was initially developed by the pharmaceutical firm Eli Lilly and was permitted by the united states Food and Drug Administration (FDA) in 1997 for the treatment of postmenopausal osteoporosis.
Another distinctive function of Evista is its capability to reduce the risk of invasive breast cancer in postmenopausal women who have osteoporosis. This was found throughout scientific trials, which confirmed a 44% discount within the risk of breast cancer among ladies taking Evista compared to these taking a placebo. This makes Evista a gorgeous option for girls who've both osteoporosis and a family historical past of breast cancer.
As with any treatment, Evista does include some potential unwanted facet effects. The commonest ones embrace scorching flashes, leg cramps, and joint ache. More serious side effects, such as blood clots, stroke, and uterine cancer, are uncommon however have been reported. It is important to discuss any concerns or potential unwanted effects with a well being care provider before beginning this medication.
One of the primary benefits of Evista is its capacity to assist prevent bone loss and enhance bone density. It works by mimicking the effects of estrogen on the bones, which helps to take care of bone strength and scale back the danger of fractures. This is very essential for postmenopausal ladies, who're at a better danger for osteoporosis as a result of lower in estrogen production.
The results of experiments on anesthetized mammalian nonmyelinated fibers support this conclusion (Ritchie and Greengard pregnancy 5 weeks ultrasound photos evista 60 mg mastercard, 1966). In these experiments, conduction could be blocked or unblocked merely by adjusting the pH of the bathing medium to 7. However, the unprotonated molecular forms also possess some anesthetic activity (Butterworth and Strichartz, 1990). The differential rate of block exhibited by fibers mediating different sensations is of considerable practical importance in the use of local anesthetics. The precise mechanisms responsible for this apparent specificity of local anesthetic action on pain fibers are not known, but several factors may contribute. However, when nerve fibers are dissected from nerves to allow direct measurement of action potential generation, no clear correlation of the concentration dependence of local anesthetic block with fiber diameter is observed (Fink and Cairns, 1984; Franz and Perry, 1974; Huang et al. Some of the vasoconstrictor agents may be absorbed systemically, occasionally to an extent sufficient to cause untoward reactions (see the next section). These effects seem to occur partly because sympathomimetic amines increase the O2 consumption of the tissue; this, together with the vasoconstriction, leads to hypoxia and local tissue damage. Ventricular tachycardia and fibrillation are relatively uncommon consequences of local anesthetics other than bupivacaine. The antiarrhythmic effects of local anesthetics such as lidocaine and procainamide are discussed in Chapter 30. Finally, it should be stressed that untoward cardiovascular effects of local anesthetic agents may result from their inadvertent intravascular administration, especially if epinephrine is also present. Smooth Muscle Local anesthetics depress contractions in the intact bowel and in strips of isolated intestine (Zipf and Dittmann, 1971). They also relax vascular and bronchial smooth muscle, although low concentrations initially may produce contraction (Covino, 1987). In general, in local anesthetics with chiral centers, the S-enantiomer is less toxic than the R-enantiomer (McClure, 1996). In general, the more potent the anesthetic, the more readily convulsions may be produced. Airway control, along with ventilatory and circulatory support, are essential features of treatment in the late stage of intoxication. Intravenously administered benzodiazepines are the drugs of choice for both the prevention and the arrest of convulsions. Whereas other local anesthetics also show the effect, cocaine has a particularly prominent effect on mood and behavior. The reaction may manifest itself as an allergic dermatitis or a typical asthmatic attack (Covino, 1987). It is important to distinguish allergic reactions from toxic side effects and from the effects of coadministered vasoconstrictors. Hypersensitivity seems to occur more frequently with local anesthetics of the ester type and frequently extends to chemically related compounds. Local anesthetic preparations containing a vasoconstrictor also may elicit allergic responses due to the sulfite added as an antioxidant for the catecholamine/vasoconstrictor. However, with prilocaine, the initial step is hydrolytic, forming o-toluidine metabolites that can cause methemoglobinemia. The extensive use of amide-linked local anesthetics in patients with severe hepatic disease requires caution. Cardiovascular System Following systemic absorption, local anesthetics act on the cardiovascular system. The rate of absorption of many local anesthetics into the systemic circulation can be considerably reduced by the incorporation of a vasoconstrictor agent in the anesthetic solution. Because toxicity is related to the concentration of free drug, binding of the anesthetic to proteins in the serum and to tissues reduces toxicity. One developing approach is promising and unusual: intravenous lipid emulsion therapy (Weinberg, 2012). Whether the lipids simply provide a favorable milieu of micelles into which lipophilic drugs can partition or the effect involves more complex biochemical pathways is not yet clear (Fettiplace et al. The amide-linked local anesthetics bind extensively (55%95%) to plasma proteins, particularly 1-acid glycoprotein. The neonate is relatively deficient in plasma proteins that bind local anesthetics and thereby is more susceptible to toxicity. Finally, reduced cardiac output slows delivery of the amide compounds to the liver, reducing their metabolism and prolonging their plasma half-lives. Lidocaine in combination with tetracaine in a formulation that generates a "peel" is approved for topical local analgesia prior to superficial dermatological procedures such as filler injections and laser-based treatments. Although it is effective when used without any vasoconstrictor, epinephrine decreases the rate of absorption, thereby decreasing the probability of toxicity and prolonging the duration of action. Both monoethylglycine xylidide and glycine xylidide retain local anesthetic activity. Ecgonine is an amino alcohol base closely related to tropine, the amino alcohol in atropine. Its high toxicity is due to reduced catecholamine uptake in both the central and peripheral nervous systems and the resulting prolongation of transmitter dwell time in the synaptic cleft. Currently, cocaine is used primarily for topical anesthesia of the upper respiratory tract, where its combination of both vasoconstrictor and local anesthetic properties provide anesthesia and shrinking of the mucosa. Lidocaine is an alternative choice for individuals sensitive to ester-type local anesthetics. Bupivacaine is more slowly absorbed than lidocaine, so plasma levels increase more slowly following a bupivacaine nerve block or epidural.
Cancer cells rom the central part o the lower lip menstrual irregularities generic evista 60 mg buy online, the foor o the mouth, and the apex o the tongue spread to the submental lymph nodes, whereas cancer cells rom lateral parts o the lower lip drain to the submandibular lymph nodes. The way in which the acial muscles alter the basic eatures is critical to communication. Lips and the shape and degree o opening o the mouth are important components o speech, but emphasis and subtleties o meaning are provided by our acial expressions. Structure o scalp: the scalp is a somewhat mobile sot tissue mantle covering the calvaria. The primary subcutaneous component o the scalp is the musculoaponeurotic epicranius to which the overlying skin is frmly attached, but it is separated rom the outer periosteum (pericranium) o the cranium by loose areolar tissue. The areolar layer enables the mobility o the scalp over the calvaria and permits traumatic separation o the scalp rom the cranium. Attachment o the skin to the epicranial aponeurosis keeps the edges o superfcial wounds together, but a wound that also penetrates the epicranial aponeurosis gaps widely. Blood may collect in the areolar space deep to the aponeurosis ater a head injury. Muscles o ace and scalp: the acial muscles play important roles as the dilators and sphincters o the portals o the alimentary (digestive), respiratory, and visual systems (oral and palpebral fssures and nostrils), controlling what enters and some o what exits rom our bodies. Other acial muscles assist the muscles o mastication by keeping ood between the teeth during chewing. Fleshy portions o the ace (eyelids and cheeks) orm dynamic containing walls or the orbits and oral cavity. Facial muscles are subcutaneous, most having a skeletal origin and a cutaneous insertion. The major terminal branches o each division reach the subcutaneous tissue o each side o the ace via three oramina that are aligned vertically. Each division supplies a distinct sensory zone, similar to a dermatome, but without the overlapping o adjacent nerves; thereore, injuries result in distinct and defned areas o paresthesia. The skin covering the angle o the mandible is innervated by the great auricular nerve, a branch o the cervical plexus. The terminal branches o the arteries o the ace anastomose reely (including anastomoses across the midline with their contralateral partners). Thus, bleeding rom acial lacerations may be diuse, with the lacerated vessel bleeding rom both ends. Most arteries o the ace are branches or derivatives o branches o the external carotid artery; the arteries arising rom the internal carotid that supply the orehead are exceptions. The arteries o the scalp are frmly embedded in the dense connective tissue overlying the epicranial aponeurosis. Thus, when lacerated, these arteries bleed rom both ends, like those o the ace, but are less able to constrict or retract than other superfcial vessels; thereore, prouse bleeding results. The veins o the ace and scalp generally accompany arteries, providing a primarily superfcial venous drainage. However, they also anastomose with the pterygoid venous plexus and with dural venous sinuses via emissary veins, which provide a potentially dangerous route or the spread o inection. Most nerves and vessels o the scalp run vertically toward the vertex; thus, a horizontal laceration may produce more neurovascular damage than a vertical one. The lymphatic drainage o most o the ace ollows the venous drainage to lymph nodes around the base o the anterior part o the head (submandibular, parotid, and superfcial cervical nodes). An exception to this pattern is the lymph drainage o the central part o the lip and chin, which initially drains to the submental lymph nodes. This fuid-lled space helps maintain the balance o extracellular fuid in the brain. This fuid leaves the ventricular system and enters the subarachnoid space between the arachnoid and pia mater, where it cushions and nourishes the brain. The two layers o the cranial dura are an external periosteal layer, ormed by the periosteum covering the internal surace o the calvaria, and an internal meningeal layer, a strong brous membrane that is continuous at the oramen magnum with the spinal dura covering the spinal cord. The external periosteal layer o dura adheres to the internal surace o the cranium. The external periosteal layer is continuous at the cranial oramina with the periosteum on the external surace o the calvaria. This outer layer is not continuous with the dura mater o the spinal cord, which consists o only a meningeal layer. The used external and internal layers o dura over the calvaria can be easily stripped rom the cranial bones. In the cranial base, the two dural layers are rmly attached and dicult to separate rom the bones. In lie, such separation at the duralcranial interace occurs only pathologically, creating an actual (blood- or fuid-lled) epidural space. It is adherent to the internal the internal meningeal layer o dura mater is a supporting layer that refects away rom the external periosteal layer o dura to orm dural inoldings (refections). The dural inoldings divide the cranial cavity into compartments, orming partial partitions (dural septa) between certain parts o the brain and providing support or other parts. The alx cerebri attaches in the median plane to the internal surace o the calvaria, rom the rontal crest o the rontal bone and crista galli o the ethmoid bone anteriorly to the internal occipital protuberance posteriorly. The tentorium cerebelli, the second largest dural inolding, is a wide crescentic septum that separates the occipital lobes o the cerebral hemispheres rom the cerebellum. The tentorium cerebelli attaches rostrally to the clinoid processes o the sphenoid, rostrolaterally to the petrous part o the temporal bone, and posterolaterally to the internal surace o the occipital bone and part o the parietal bone. The alx cerebri attaches to the tentorium cerebelli and holds it up, giving it a tent-like appearance (L. The tentorium cerebelli divides the cranial cavity into supratentorial and inratentorial compartments. The supratentorial compartment is divided into right and let halves by the alx cerebri.
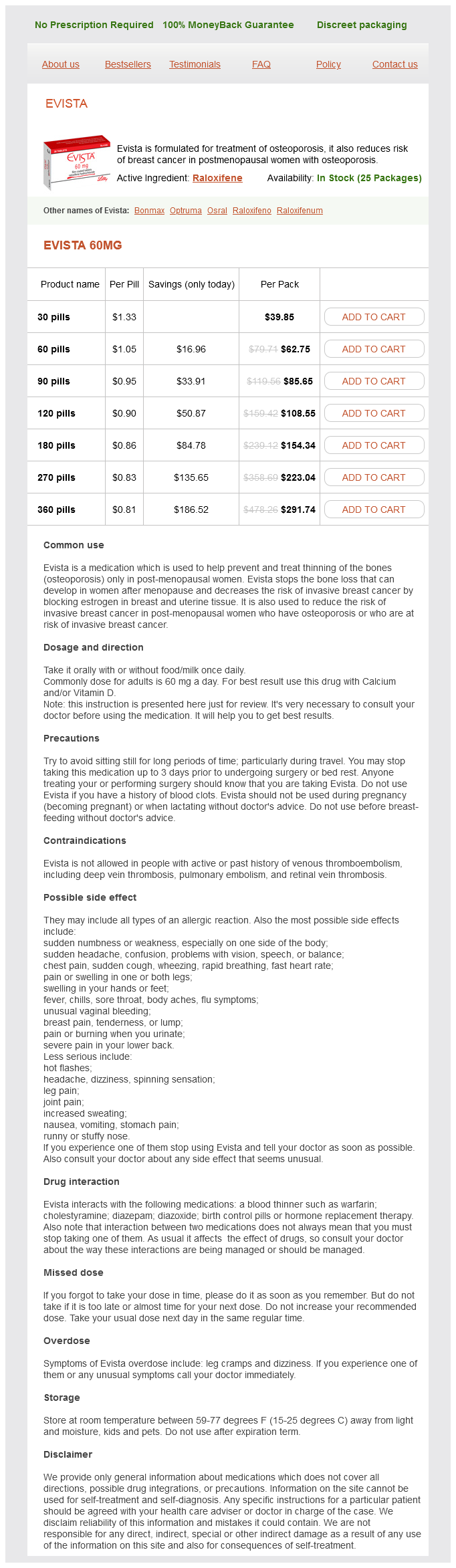
Evista Dosage and Price
Evista 60mg
- 30 pills - $39.85
- 60 pills - $62.75
- 90 pills - $85.65
- 120 pills - $108.55
- 180 pills - $154.34
- 270 pills - $223.04
- 360 pills - $291.74
The foor o the duct is also ormed by part o the duct women's health center new prague mn purchase evista paypal, the basilar membrane, plus the outer edge o the osseous spiral lamina. The receptor o auditory stimuli is the spiral organ (o Corti), situated on the basilar membrane. The spiral organ contains hair cells, the tips o which are embedded in the tectorial membrane. The organ is stimulated to respond by deormation o the cochlear duct induced by the hydraulic pressure waves in the perilymph, which ascend and descend in the surrounding scalae vestibuli and tympani. The cell bodies o the primary sensory neurons are in the spiral (cochlear) ganglion, located at the root o the spiral lamina o the cochlea. The internal acoustic meatus opening is in the posteromedial part o this bone, in line with the external acoustic meatus. The internal acoustic meatus is closed laterally by a thin, perorated plate o bone that separates it rom the internal ear. The vestibulocochlear nerve divides near the lateral end o the internal acoustic meatus into two parts: a cochlear nerve and a vestibular nerve. A localized collection o blood orms between the perichondrium and auricular cartilage, causing distortion o the contours o the auricle. Acute Otitis Externa Otitis externa is an infammation o the external acoustic meatus. The inection oten develops in swimmers who do not dry their meatus (ear canals) ater swimming and/or use ear drops. Otoscopic Examination Examination o the external acoustic meatus and tympanic membrane begins by straightening the meatus. These movements reduce the curvature o the external acoustic meatus, acilitating insertion o the otoscope. The meatus is relatively short in inants; thereore, extra care must be exercised to prevent injury to the tympanic membrane. The meatus is straightened in inants by pulling the auricle ineroposteriorly (down and back). The examination also provides a clue to tenderness, which can indicate infammation o the auricle and/or the meatus. The handle o the malleus is usually visible near the center o the membrane (the umbo). Otitis Media An earache and a bulging red tympanic membrane may indicate there is pus or fuid in the middle ear, which is a sign o otitis media. Infammation and swelling o the mucous membrane lining the tympanic cavity may cause partial or complete blockage o the pharyngotympanic tube. The tympanic membrane becomes red and bulges, and the person may complain o "ear popping" or crackling. I untreated, otitis media may produce impaired hearing owing to scarring o the auditory ossicles, limiting their ability to move in response to sound. Peroration may also result rom oreign bodies in the external acoustic meatus, trauma, or excessive pressure. Because the superior hal o the tympanic membrane is much more vascular than the inerior hal, incisions to release pus rom a middle ear abscess (myringotomy), or example, are made postero-ineriorly through the membrane. During operations or mastoiditis, surgeons are conscious o the course o the acial nerve to avoid injuring it. In children, only a thin plate o bone must be removed rom the lateral wall o the antrum to expose the tympanic cavity. Blockage o Pharyngotympanic Tube the pharyngotympanic tube orms a route or an inection to pass rom the nasopharynx to the tympanic cavity. This tube is easily blocked by swelling o its mucous membrane, even as a result o mild inections. When the pharyngotympanic tube is occluded, residual air in the tympanic cavity is usually absorbed into the mucosal blood vessels, resulting in lower pressure in the tympanic cavity, retraction o the tympanic membrane, and intererence with its ree movement. Mastoiditis Inections o the mastoid antrum and mastoid cells (mastoiditis) result rom a middle ear inection that causes inlammation o the mastoid process. Inections may spread superiorly 8 Paralysis o Stapedius the tympanic muscles have a protective action in that they dampen large vibrations o the tympanic membrane resulting rom loud noises. Under the inluence o gravity, the otoliths cause bending o the hair cells, which stimulate the vestibular nerve, and provide awareness o the position o the head in space; the hairs also respond to quick tilting movements and to linear acceleration and deceleration. Motion sickness results rom discordance between vestibular and visual stimulation. External coil Internal coil Ground electrode in epitympanic recess Cochlear nerve Cochlea Microphone Tympanic membrane Stimulator wire from microphone to speech processor Stimulator wire from speech processor to external coil Active electrode Dizziness and Hearing Loss Injuries o the peripheral auditory system cause three major symptoms: hearing loss (usually conductive hearing loss), vertigo (dizziness) when the injury involves the semicircular ducts, and tinnitus (buzzing or ringing) when the injury is localized in the cochlear duct. Tinnitus and hearing loss may result rom lesions anywhere in the peripheral or central auditory pathways. The two types o hearing loss are as ollows: Conductive hearing loss: resulting rom anything in the external or middle ear that intereres with conduction o sound or movement o the oval or round windows. People with this type o hearing loss oten speak with a sot voice because, to them, their own voices sound louder than background sounds. Sensorineural hearing loss: resulting rom deects in the pathway rom the cochlea to the brain: deects o the cochlea, cochlear nerve, brainstem, or cortical connections. Cochlear implants are one approach employed to restore sound perception when the hair cells o the spiral organ have been damaged.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.