
Extra Super Levitra
General Information about Extra Super Levitra
In conclusion, Extra Super Levitra is an excellent treatment option for men struggling with each ED and PE. It provides a convenient and efficient resolution to two frequent male sexual dysfunctions, serving to men regain their confidence and satisfaction in the bed room. With the combination of Vardenafil and Dapoxetine, Extra Super Levitra provides a powerful solution to enhance sexual performance and improve the general quality of life for males.
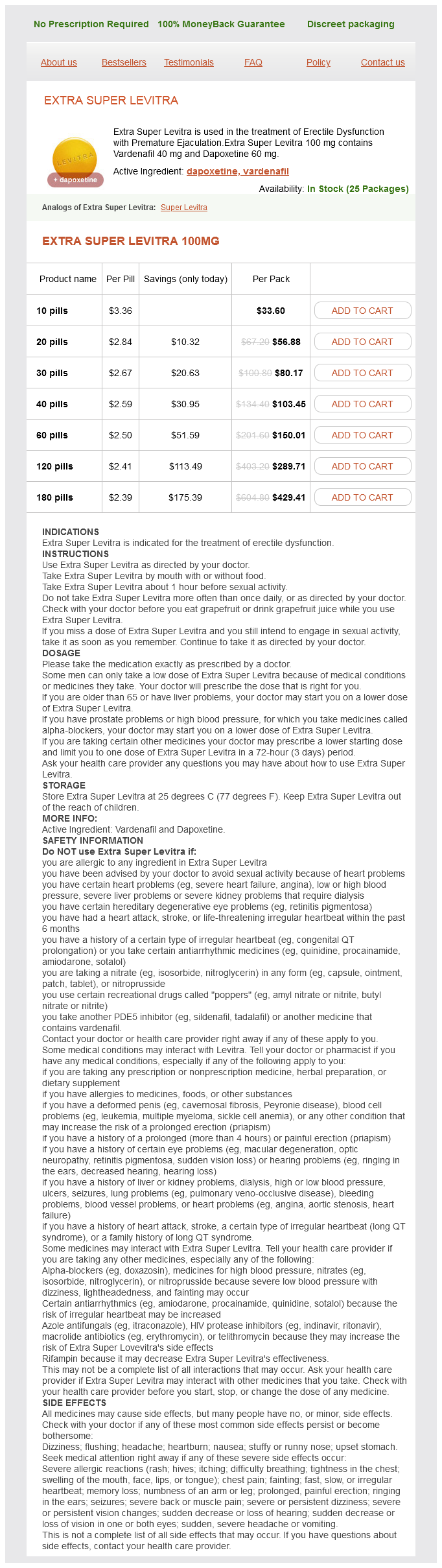
Extra Super Levitra is a revolutionary medicine designed to deal with two common male sexual dysfunctions: erectile dysfunction (ED) and untimely ejaculation (PE). This advanced medicine incorporates a mixture of Vardenafil and Dapoxetine, making it highly efficient in helping males overcome these two points and obtain a more fulfilling sex life.
Extra Super Levitra can be purchased with a prescription from a health care provider or by way of many on-line pharmacies. It is necessary to seek the advice of with a healthcare professional earlier than taking this treatment, as it could interact with sure medicines and is not appropriate for men with certain medical circumstances.
Dapoxetine, however, is a selective serotonin reuptake inhibitor (SSRI) that's commonly used to deal with PE. It works by rising the degrees of serotonin within the brain, which helps to delay ejaculation and enhance management over ejaculation. Dapoxetine has been extensively studied and has been discovered to significantly increase the time taken for ejaculation, allowing men to last more in mattress.
Extra Super Levitra is a game-changer for men suffering from these two situations. It combines the power of two lively elements, Vardenafil and Dapoxetine, to deliver distinctive ends in the remedy of ED and PE. Vardenafil belongs to a class of medications referred to as phosphodiesterase sort 5 (PDE5) inhibitors, which work by rising blood move to the penis, permitting for a firm and long-lasting erection. It is the same active ingredient found within the well-liked ED treatment, Levitra.
This treatment has been clinically proven to be extremely effective in treating each ED and PE. In a study of over 2,500 men, Extra Super Levitra was found to considerably improve erectile function, enhance the time to ejaculation, and improve overall sexual satisfaction. It has also been confirmed to be protected and well-tolerated, with minimal unwanted effects corresponding to headache, dizziness, and nausea.
Extra Super Levitra is available in a tablet form, with every pill containing 100 mg of Vardenafil and 60 mg of Dapoxetine. The beneficial dose is one pill, taken orally with a glass of water, about half-hour before sexual exercise. It is really helpful to take no more than one tablet per day to avoid any potential unwanted facet effects.
Erectile dysfunction is a situation where a man is unable to get or keep an erection during sexual exercise. It can have numerous causes, such as stress, anxiousness, or underlying health situations. On the other hand, untimely ejaculation is a situation the place a person ejaculates within a minute of sexual activity, typically leaving each companions unsatisfied. It could cause distress, low self-esteem and can pressure relationships.
Also erectile dysfunction causes high blood pressure cheap extra super levitra 100 mg with mastercard, the presence of stereocilia, a typical feature, is consistent with an absorptive function. Areas of apical cell cytoplasm that protrude out between stereocilia are called apical blebs and function in apocrine secretion. The secretory protein is thought to interact with spermatozoa and affect their mobility. The presence of abundant vesicles and vacuoles in apical cytoplasm correlates with endocytosis, which occurs at the apical surface. Colliculus Urethral crest Cavernous urethra Prostate Utricle Ejaculatory duct orifice Cowper gland Urogenital diaphragm Membranous urethra Openings of Cowper gland ducts Histology of prostate. Ureter Vas deferens Seminal vesicle Ampulla of vas Ischiopubic ramus Superior fascia of urogenital diaphragm Muscles of urogenital diaphragm Prostate Cowper glands Fibromuscular stroma Transitional zone Central zone Urethra Peripheral zone Ampulla vas deferens Seminal vesicle Prostate transverse section. It is covered by a thin, indistinct fibroelastic connective tissue capsule mixed with smooth muscle and is traversed posteriorly by ejaculatory ducts. The prostate, a collection of up to 50 compound tubuloalveolar glands, has traditionally been divided anatomically into several lobes. Because the lobes are indistinct and some organs may be atrophic in normal adult humans, the prostate is better divided into three concentric zones, which are best seen in the sagittal plane. The central zone represents 25% of the prostate and consists of submucosal glands. This pattern has clinical significance: in most cases benign prostatic hyperplasia arises in the transitional zone; the peripheral zone is the one most susceptible to inflammation and the site of most prostatic adenocarcinomas. Their ducts fuse with the distal end of the paired ductus deferens to form ejaculatory ducts, which enter the prostate and end in the prostatic urethra. Radical prostatectomy (retropubic, laparoscopic, or perineal) surgically removes the entire prostate, seminal vesicles, and periprostatic tissue. In some cases, regional pelvic lymph nodes are removed to determine whether metastasis has occurred. After prostate excision, the neck of the urinary bladder is reconstructed and anastomosed to urethra. In some patients, major side effects are erectile dysfunction and urinary incontinence. Brachytherapy-less invasive with lower risk of complications-utilizes rice-sized radioactive "seeds" (iodine-105, palladium-103, cesium-137, iridium-192) implanted directly into tumor site with aim of destroying cancer cells. Columnar epithelial cells, which have lightly stained apical cytoplasm, line A prostatic concretion (*) is in the alveolar lumen. The adult prostate is made of numerous individual tubuloalveolar glandular units, irregularly shaped, that open by separate branching ducts into the prostatic urethra. They are embedded in fibromuscular stroma, dense with collagen and irregularly arranged smooth muscle. The secretory nature of the glandular epithelium is clear at high magnification: the pseudostratified epithelium has both basal and secretory cells. With aging, prostatic concretions (corpora amylacea)-ovoid, eosinophilic, concentrically lamellated bodies-may be found in alveolar lumina. They are thought to be a mixture of prostatic secretions and debris from degenerated epithelial cells. Testosterone may cause the glandular component of the prostate to undergo hyperplasia and hypertrophy. Symptoms are frequent or painful urination (dysuria), pelvic pain, fever, and sexual dysfunction; the diagnosis is via rectal digital examination, blood culture, and urinalysis. Histologically, polymorphonuclear leukocytes typically infiltrate prostatic alveoli and surrounding stroma. The secretory nature of the columnar epithelial cells is clear, even if individual cell borders are difficult to distinguish. A prominent Golgi complex in the supranuclear region of each cell gives rise to membrane-bound secretory vacuoles and vesicles, which are pleomorphic, vary in size, and may appear empty or contain flocculent or electron-dense material. In the Golgi complex, secretory products are modified and then sorted into secretory vesicles destined for the cell surface. After fusion with the apical cell membrane, secretory vesicles and vacuoles release their contents into the lumen. Cytologic features include hyperchromatic enlarged nuclei in secretory epithelium and absence of the basal cell layer. Causes remain uncertain, but androgens are thought to influence the pathogenesis, and several risk factors including age, race, and family history may play a role in etiology. The honeycombed mucosa has an epithelium (arrows) composed of columnar cells and basal cells. Semen consists of spermatozoa formed in germinal epithelium of the testis and seminal fluid, the components of which are secreted by the excretory duct system and accessory glands. The epithelium is usually pseudostratified, but it may be simple columnar in places. These convoluted tubulosaccular glands have internal folds of connective tissue forming crests and ridges lined by secretory epithelium projecting into the lumen. In histologic sections, the large lumen comprises separate cavities of various sizes, which communicate with each other throughout the gland. The lumen contains coagulated eosinophilic material thought to be stored secretion. Like the prostate, seminal vesicles depend on androgen and develop fully only after puberty. The epithelium, like that in other areas of the male reproductive tract, is mostly pseudostratified with basal cells and columnar cells. By electron microscopy, polarized columnar cells show features typical of secretory epithelium-well-developed Golgi complex, abundant rough endoplasmic reticulum, numerous mitochondria, and apical secretory vesicles.
An outer tunic erectile dysfunction when drugs don't work proven extra super levitra 100 mg, the adventitia, is fibrous connective tissue and is known as a serosa in areas in the peritoneal cavity, where this outer tunic is covered externally by peritoneal mesothelium. It has many causes; disorders leading to it may affect oral, pharyngeal, or esophageal phases of swallowing. Esophageal stricture (or peptic stenosis) is a common diagnosis in patients with esophageal dysphagia, often resulting from scar tissue formation. Usually a complication of gastroesophageal reflux disease, it may also be caused by esophagitis (inflammation of the esophagus), hiatus hernia, or dysfunctional motility. Diagnostic tests include upper endoscopy, fiberoptic evaluation of swallowing, and barium esophagography. The highly corrugated interface between epithelium and connective tissue shows tall papillae (*) penetrating the epithelium to take capillaries close to the surface. Right, the external cutaneous surface, of typical thin skin, consists of epidermis (Ep) and underlying dermis (De). Each lip has three surfaces: an outer cutaneous part, red (vermilion) border, and inner oral mucosa. Like thin skin in other parts of the body, it consists of an epidermis and an underlying dermis with hair follicles, sebaceous glands, and sweat glands. A transitional zone between skin and oral mucosa is the free edge, or vermilion border. Its stratified squamous epithelium is thick and either lacks a superficial layer of keratin or is lightly keratinized. Under the epithelium are tall connective tissue papillae that are close to the surface. The vermilion border is pinkish-red because of the relatively translucent epithelium and the blood in capillaries in the papillae. The lower lip is prone to these neoplasms, usually caused by chronic sun exposure, and middle-aged and elderly men are more susceptible to them than women. Compared with other head and neck cancers, lip carcinoma is readily curable, but sometimes regional metastasis, local recurrence, and death may occur. Treatment involves equally effective surgical excision or radiation therapy, the choice depending on tumor size. The connection of the duct is not seen in the plane of section, but it opens onto Lip mucocele. These papillae resemble those under the epidermis but are thinner and more delicate. The highly corrugated interface between epithelium and lamina propria firmly anchors these tissues against mechanical forces such as friction. The lamina propria contains collagen and elastic fibers, which permit distensibility over underlying tissues. It also harbors capillaries and lymphatics plus many lymphocytes and other cells, which aid in immunologic defense against pathogens and irritants in the external environment. Surface cells of the epithelium are continuously shed into the oral cavity lumen, the renewal rate of these cells being 12-14 days. As in other epithelia, a basement membrane separates its basal aspect from the lamina propria. Small groups of minor salivary glands, the labial glands, are deep to the lamina propria in the submucosa. Secretions of these mainly mucus-secreting exocrine glands drain onto the oral surface via small ducts, thereby providing moisture and lubrication. The bulk of the lip is made of a central core of skeletal muscle, the orbicularis oris muscle, whose fibers are surrounded by fibroelastic connective tissue. Lining mucosa forms the inner lining of the lips, cheeks, soft palate, floor of the mouth, and undersurface of the tongue. It is mainly nonkeratinized stratified squamous epithelium with underlying, supportive lamina propria. Masticatory mucosa consists of stratified squamous epithelium that is lightly keratinized (cells in the stratum corneum retain nuclei). Specialized mucosa on the dorsal surface of the tongue has many papillae and taste buds. The lamina propria, with short papillae and abundant elastic fibers, attaches at intervals to underlying skeletal muscle fibers of the buccinator. These fibers are arranged into fascicles that mix with minor salivary (buccal) glands. The gingiva, a mucous membrane that lacks glands, covers outer and inner surfaces of the alveolar processes of the maxilla and mandible and surrounds each tooth. Its stratified squamous epithelium overlying a thick, fibrous lamina propria is lightly keratinized on its surface and lacks a stratum granulosum. The lamina propria is firmly anchored to underlying periosteum of the bone, which makes the mucosa immobile and inelastic. The lamina propria extends into deep papillary projections into the base of the epithelium. As in other areas of the oral cavity, papillae contain a large network of capillaries. Gingivitis is usually caused by accumulation of plaque or calculus (tartar), containing large numbers of bacteria. Bacterial invasion of the oral mucosa leads to swelling, irritation, bleeding, and redness of gums. Features of chronic gingivitis include accumulation of plasma cells and B lymphocytes in the lamina propria, plus destruction of collagen. Untreated, gingivitis may lead to more serious complications such as periodontitis.
Extra Super Levitra Dosage and Price
Extra Super Levitra 100mg
- 10 pills - $33.60
- 20 pills - $56.88
- 30 pills - $80.17
- 40 pills - $103.45
- 60 pills - $150.01
- 120 pills - $289.71
- 180 pills - $429.41
The vesicles may store acetylcholine erectile dysfunction caused by hemorrhoids order extra super levitra 100 mg overnight delivery, norepinephrine, or other neurotransmitters before release. In some sites, smooth muscle cells are individually innervated by efferent nerve endings. In most areas, however, not all smooth muscle cells are innervated, and the branch of an autonomic nerve fiber supplies groups of several cells. Gap junctions between cells allow excitation to spread among adjacent cells, which results in synchronous contractions. Circulating hormones such as oxytocin stimulate contraction in the uterus during birth, and local substances such as histamine and serotonin or physical factors such as stretching can affect muscle activity. Asthma and hypertension are often due to sustained contraction of bronchial and vascular smooth muscle, respectively. Excess histamine in allergy, for example, frequently induces increased excitation of smooth muscle activity, thereby narrowing the airways. In atherosclerosis, arterial smooth muscle cells accumulate cholesterol, which often leads to formation of plaques that compromise normal blood flow. Many therapeutic drugs, such as bronchodilators and vasodilators, influence contractile regulatory mechanisms affecting smooth muscle. Gross appearance with rupture of left ventricle, seen in posterior view (left) and coronal section (below) of heart. Distinct aggregations of inflammatory cells are present around a necrotic region of myocardium. Cardiac muscle cells show early necrosis: being smudged and eosinophilic with loss of cross-striations; many appear as "wavy fibers" (Upper Right) that are narrow and elongated. Men are more at risk than women throughout life, but it is the leading cause of death in elderly women. Caused by severe prolonged ischemia (loss of blood supply) to myocardium, it leads to loss of cardiac contractility and death (necrosis) of cardiac muscle cells. Symptoms include chest pain (often radiating to the arms or neck), fatigue, palpitations, and shortness of breath (dyspnea). Initial ultrastructural changes of muscle cell necrosis are disruption of the sarolemmal membrane, glycogen depletion, and mitochondrial swelling. Key features of myocyte necrosis are "wavy" fibers, loss of cross-striations, contraction bands, pyknosis, and loss of nuclei (karyolysis). These changes are accompanied by interstitial edema, hemorrhage, macrophage infiltration, appearance of fibrovascular granulation tissue, and myocardial fibrosis. Its sympathetic and parasympathetic portions innervate organs and tissues that are under autonomic, or involuntary, control such as glands, smooth muscle, and cardiac muscle. Neurons can generate nervous impulses in response to stimuli and transmit them along cellular processes. The types of neurons are classified on the basis of appearance, shape, and number of processes as multipolar, bipolar, or pseudounipolar. Despite their variability, all neurons conform to a common histologic plan: highly specialized cells with several parts to carry out functions of receiving signals and then transmitting information as nerve impulses to other neurons or effector organs. Conductivity and irritability are best developed in neurons; glial cells are non-impulse-conducting cells that represent interstitial tissue and mostly support and protect neurons. Nervous Tissue Neural plate of forebrain Neural groove Neural folds 1st occipital somite Future neural crest Neural plate 111 Ectoderm Level of section Ectoderm Neural crest Future neural crest Fused neural folds Neural fold 1st occipital somite 1st cervical somite 1st thoracic somite Level of section Neural tube Level of section Primitive streak Neural plate of forebrain Neural groove Neural folds Fused neural folds 1st cervical somite Caudal neuropore Level of section Embryo at 20 days. Neural groove Neural crest Sulcus limitans Caudal neuropore Embryo at 24 days (dorsal view). Meningocele Meningomyelocele Types of spina bifida with protrusion of spinal contents. Incomplete closure of the embryonic neural tube (typically at L4-S1 levels) leads to clinical symptoms that vary widely in severity. It becomes indented and forms a longitudinal neural groove with neural folds on each side. Isolated cells not incorporated into the neural tube form a strip of neuroectodermal cells-the neural crest. These cells migrate ventrolaterally along each side of the neural tube to form a series of somites. The neural tube lumen gives rise to fluid-filled ventricles of the brain and central canal of the spinal cord. They are composed of three distinct layers: an outermost dura mater, arachnoid, and innermost pia mater. Anencephaly is a congenital malformation caused by failure of fusion of neural folds in rostral regions. Degeneration of unfused folds leads to failure of development of neural tissue and absence of most of the brain, the result being stillbirth or premature death. A defect at more caudal levels of the primitive spinal cord is called spina bifida. This condition typically produces paralysis depending on the level of the lesion and is usually not life-threatening. Underlying the arachnoid (Ar), a more delicate connective tissue, is the subarachnoid space (*), which, in life, contains cerebrospinal fluid. The thickest and toughest layer, the dura, is dense, fibrous connective tissue consisting of interlacing bundles of collagen and elastic fibers associated with flattened fibroblasts. The outer aspect of the dura attaches to the periosteum of the skull; the inner dural surface is lined by a layer of flattened fibroblasts. Two potential spaces associated with it are the epidural space (exterior) and subdural space (between dura and arachnoid). These normally potential spaces can in some pathologic conditions accumulate fluid such as blood.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.