
Kamagra Effervescent
General Information about Kamagra Effervescent
Another benefit of Kamagra Effervescent is that it is straightforward to take. As mentioned earlier, the tablets dissolve in water, making it best for individuals who struggle with swallowing pills. This also implies that the treatment may be taken discreetly, with out the need for water or anybody noticing, making it a convenient possibility for men who may be self-conscious about their situation.
In addition to its efficacy, Kamagra Effervescent is also recognized for its affordability. As the generic model of Viagra, it's rather more cost-effective, making it a extra accessible possibility for lots of males. This is particularly useful for those who could have to take the medication regularly and for an extended period, as it could be a more economical alternative in the long run.
As with any medication, there are some potential side effects associated with Kamagra Effervescent. These can embrace headache, dizziness, nausea, flushing, and changes in vision. These unwanted facet effects are normally gentle and momentary, but if they persist or turn into extreme, you will want to search medical attention.
Fortunately, there are numerous therapy options available for erectile dysfunction, considered one of which is Kamagra Effervescent. It is an innovative treatment that has gained recognition for its effectiveness in treating this condition. In this text, we'll take a more in-depth have a look at what Kamagra Effervescent is, how it works, and its benefits.
Erectile dysfunction, also called impotence, is a common medical situation that affects hundreds of thousands of males everywhere in the world. It is outlined as the inability to attain or keep an erection adequate for sexual activity. While most men expertise occasional difficulties with erections, persistent erectile dysfunction can have a big impact on a person's self-esteem, relationships, and total high quality of life.
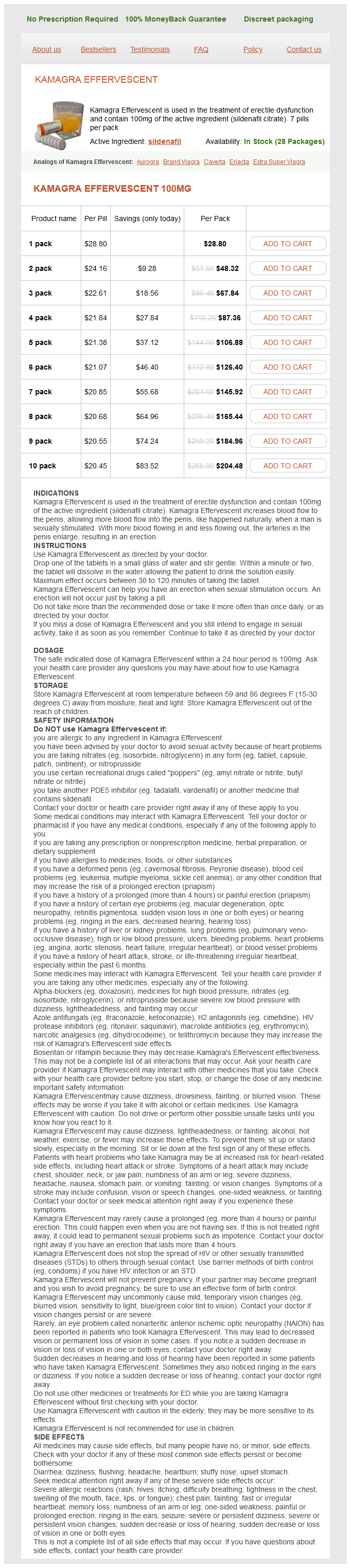
Kamagra Effervescent is a drugs used for the therapy of erectile dysfunction. It accommodates 100mg of the lively ingredient sildenafil citrate, which can be found within the popular treatment Viagra. This lively ingredient works by growing the blood move to the penis, which helps to achieve and maintain an erection. Kamagra Effervescent comes within the type of tablets that dissolve in water, making it easier for men who've issue swallowing drugs.
In conclusion, Kamagra Effervescent is a well-liked and effective treatment possibility for erectile dysfunction. With its fast-acting and long-lasting results, affordability, and ease of use, it has helped many males regain their sexual confidence and improve their general high quality of life. However, you will want to consult with a doctor earlier than beginning any new medicine to make sure it's the right alternative for you and to attenuate any potential dangers.
One of the primary advantages of Kamagra Effervescent is that it acts quickly, typically inside 30 minutes to an hour after consumption. This makes it a popular alternative for men who need a fast-acting solution for their erectile dysfunction. The treatment also has an extended length of motion compared to different drugs, lasting up to 4-6 hours. This prolonged window of effectiveness permits for more flexibility and spontaneity in sexual actions, giving men extra control over their sexual well being.
It is important to note that Kamagra Effervescent ought to solely be taken as directed by a well being care provider. It isn't suitable for everybody, and there are particular medical circumstances and drugs that may interact with it and trigger antagonistic effects. It can be essential to avoid taking the medication with alcohol or grapefruit juice, as it might enhance the risk of unwanted effects.
Longer follow-up of this population confirms these data and suggests that early response to therapy is predictive of a good long-term outcome and that the long-term results are excellent erectile dysfunction protocol free ebook generic kamagra effervescent 100 mg buy online. Treatment failures, relapses following therapy, discontinuations of therapy, mortality, and time to remission were similar. The calcineurin inhibitors cyclosporine and tacrolimus have been proven to increase the induction remission rate in a number of uncontrolled and controlled trials. A recent large multicenter trial from China of more than 350 patients showed equally good results with this multitargeted therapy. It continues to be used in patients resistant to other treatments and in those who do not tolerate conventional treatment. Likewise, plasmapheresis synchronized to intravenous cyclophosphamide pulse therapy has not proven effective. Thus, early trials reported low and inconsistent response rates with oral corticosteroids. At 3 years only 12% had relapsed, at 5 years only 16%, and at 90 months only 19% had relapsed. Clearly in this population a regimen of steroids plus azathioprine was highly effective. Lupus patients have accelerated atherogenesis and a disproportionate rate of coronary vascular disease, leading to a high mortality rate. In addition, use of calcium, vitamin D supplements, and bisphosphonates to prevent glucocorticoid-induced osteoporosis may be useful. Some form of antiphospholipid antibodies is present in 40% to 75% of lupus patients. However, some would recommend low-dose aspirin and hydroxychloroquine for prophylaxis of asymptomatic patients with antiphospholipid antibodies. In patients with evidence of a clinical thrombotic event, most investigators use chronic anticoagulation with warfarin as long as the antibody persists. The antibody-positive patients also had a greater incidence of chronic renal failure than the antibodynegative patients. They may include IgG and/or IgM anticardiolipin antibodies, antibodies to 2-glycoprotein I of IgG or IgM isotype, or lupus anticoagulant activity. Thrombocytopenia and prolonged partial thromboplastin time are frequent laboratory findings. The presence of antiphospholipid antibodies should be documented on two or more occasions at least 12 weeks apart and within 5 years of clinical manifestations. They may also impair fibrinolysis through inhibition of such factors as tissue type plasminogen activator. Patients with IgG anticardiolipin antibodies again had a higher incidence of thromboses, as did those with a lupus anticoagulant. A retrospective renal biopsy study found antiphospholipid nephropathy in almost 40% of antiphospholipid-positive patients versus only 4% of patients without antiphospholipid antibody. When antiphospholipid nephropathy was present, it was associated with both lupus anticoagulant and anticardiolipin antibodies. Therapy of this glomerular lesion clearly differs from that of immune complexmediated glomerulonephritis. There is a high prevalence of antiphospholipid antibodies (10% to 30%) in hemodialysis patients irrespective of patient age, gender, or duration of the dialysis. Bleeding complications occurred in 29 of the 147 patients but were severe in only 7 patients. Other patients have focal proliferative glomerulonephritis with both mesangial and subendothelial deposits, but fibrinoid necrosis and crescents are rare. The most common pattern of glomerular involvement is membranous nephropathy, reported in up to 35% of cases,241,243-245 with typical peripheral capillary wall granular immunofluorescence staining for IgG, C3, and, at times, IgA and IgM. Some patients will have a mixed pattern of membranous plus mesangial proliferative glomerulonephritis. By ultrastructure analysis, lupus-like findings have been reported, including endothelial tubuloreticular inclusions, deposits with "fingerprint" substructure, and tubular basement membrane deposits. In autopsy series, in which two thirds of patients had clinical renal disease, a similar distribution of glomerular lesions was found. Intravenous immunoglobulin has been used to treat thrombocytopenia and hemolytic anemia. Global proliferation and necrotizing glomerular tuft involvement are more common in the more severe cases. The earliest lesions are "intracapillary thrombosis" with deposition of eosinophilic "fibrinoid" material associated with endothelial cell swelling, infiltration by polymorphonuclear leukocytes, and pyknosis or karyorrhexis. There is considerable overlap in the clinical, histologic, and laboratory features of these entities. However, genetic analyses are defining differences between these entities, and differences in the course and response to therapy are being noted. True electron-dense immune-type deposits are not usually identified and, when present, are sparse and illdefined. Chronic segmental or global glomerulosclerosis with fibrous crescents often occur side by side with more active glomerular lesions. Tubules show focal degenerative and regenerative changes, and cortical infarcts may occur. Granulomas containing giant cells may form in the interstitium of the cortex and medulla in 3% to 20% of cases. Some of these cortical granulomas represent foci of glomerular destruction by granulomatous crescents. Papillary necrosis, often bilateral and affecting most papillae, has been reported, usually in those with necrotizing interstitial capillaritis of the vasa recta.
In 2003 erectile dysfunction hiv best kamagra effervescent 100 mg, the College of American Pathologists conducted a survey of 5624 participating laboratories that showed a bias from the reference value of between -0. As a result a creatinine standard reference material was prepared by the National Institute of Standards and Technology, which is currently being used by almost all major manufacturers for calibration. The Jaffe method measures creatinine by complexing creatinine with alkaline picrate, followed by measurement with a colorimetric technique. This colorimetric assay may falsely measure normal plasma constituents such as glucose and plasma proteins as creatinine. The Jaffe method may also report falsely low creatinine levels if there are very high serum bilirubin levels. Modified Jaffe methods attempt to take this into account by removing these interfering chromogens before analysis. This inference is sometimes corrected for by some manufacturers by deducting an estimated value based on average bias from measured results. Currently, the techniques used in most laboratories are modified alkaline picrate and enzymatic methods, but it is recommended that the enzymatic method be adopted because this is more specific. This error was previously compensated for by errors in the Jaffe assay that would overestimate serum creatinine value. The main problem with creatinine clearance is its reliance on timed urine collection, which is often inaccurate. Volume status should be taken into account because dilution of creatinine leads to an apparently low result. With the equation discussed earlier to calculate clearance of a filtration marker, CrCl is calculated as follows: CrCl = Urine concentration × urine volume Plasma concentration × time For example, for a patient with a serum creatinine value of 100 µmol/L, a urine creatinine value of 10,000 µmol/L, and a urine volume of 1. It is freely filtered by the kidney and is not secreted; proximal tubule cells reabsorb and catabolize the filtered cystatin C so that little is normally excreted in the urine. Rather, urinary cystatin C has been regarded as one of several available markers of kidney injury and may be found in the urine during glomerular injury with heavy proteinuria. Plasma cystatin C levels are highest in the first days of life and stabilize after age 1 year, with levels approximating those of adults. This is problematic as, for example, cystatin C may not be useful in renal transplant patients because they have subclinical inflammation and commonly use long-term corticosteroids. Other techniques are radioimmunoassay, fluorescent techniques, and enzymatic immunoassays. At the writing of this chapter, the measurement of serum cystatin C is not internationally standardized. A reference material was produced in 2010, and manufacturers are in the process of recalibrating their assays against this standard. The adoption of serum cystatin C in place of serum creatinine at present is made difficult predominantly by the expense of the assay, variation in production, and absence of universal assay standardization. Novel Endogenous Filtration Markers Several alternative novel endogenous substances are under investigation as potential markers that could be used aside from urea, creatinine and cystatin C. The performance of estimation equations is assessed by measurements of bias, precision, and accuracy. Modification of Diet in Renal Disease and Chronic Kidney Disease Epidemiology Collaboration Equations. A number of coefficients have been derived to compensate for differences in body mass and diet in populations of different ethnicity with varying degrees of performance. Cystatin C measurement in the derivation of these equations was traceable to the standard reference material for cystatin C, although cystatin C measurement is not uniformly standardized, as noted previously. This difference in ability to risk-stratify is due to the different degrees of importance placed on factors such as age and sex, which also affect prognosis, in these equations. This equation was developed in 1976 from a cohort of 249 men, and the creatinine assay method that was used to derive this equation was not standardized. Inulin is a polymer of fructose found in tubers such as the Jerusalem artichoke and chicory. It distributes in extracellular fluid, does not bind to plasma proteins, is freely filtered at the glomerulus, and is neither reabsorbed nor secreted by the renal tubules. Inulin is intravenously infused at a constant rate while blood and urine are sampled frequently over several hours, ideally following insertion of a bladder catheter. The patient takes an oral water load and must continue consuming water throughout the test to ensure a high urine output. Clearance Methods for Other Exogenous Filtration Markers Owing to the difficulty and expense of using inulin, new reference standard filtration markers have been introduced as alternatives and have been widely used since the 1990s. Clearance of these filtration markers can be measured in the urine or in blood or with nuclear imaging in the case of radiolabeled markers to avoid problems with urine collection. The decline in serum levels is due initially to the disappearance of the marker from the plasma into its volume of distribution (fast component) and then subsequently to renal excretion (slow component). It is best estimated using a two-compartment model that requires blood sampling early (usually two or three time points until 60 minutes) and late (one to three time points from 120 minutes onward). X-ray fluorescence of samples may also be used to measure iodine levels but requires a higher dose of contrast agent. It is not reabsorbed, metabolized, or secreted by the kidney and is excreted completely nonmetabolized in the urine. Urinary clearances of iothalamate and iohexol closely correlate with urinary inulin clearance, and there is a high correlation among the methods.
Kamagra Effervescent Dosage and Price
Kamagra Effervescent 100mg
- 1 pack - $28.80
- 2 pack - $48.32
- 3 pack - $67.84
- 4 pack - $87.36
- 5 pack - $106.88
- 6 pack - $126.40
- 7 pack - $145.92
- 8 pack - $165.44
- 9 pack - $184.96
- 10 pack - $204.48
Goodpasture antibodies breach only the quaternary structure of hexamers containing only monomer subunits generic erectile dysfunction drugs in canada cheap kamagra effervescent online visa, whereas hexamers composed of both dimer and monomer subunits (D-hexamers) are resistant to autoantibodies under native conditions. Investigations using this model suggest that the terminal components of the complement system are not involved in the pathogenesis of disease. Both protective effects could be overcome if the dose of nephritogenic antibodies was increased. C1q- and C4-deficient mice did develop proteinuria, which is suggestive of involvement of the alternative complement pathway. Prompt treatment with plasmapheresis, corticosteroids, and cyclophosphamide results in patient survival of approximately 85% and renal survival of approximately 60%. The usual pulmonary manifestation is severe pulmonary hemorrhage, which may be life threatening; however, patients may have milder disease that can be focal. For patients with early or focal disease, a high level of suspicion is necessary to establish the diagnosis, especially in the presence of unexplained anemia. The diagnosis may be aided by measurements showing an increased diffusing capacity of carbon monoxide and by findings on computed tomography of the chest. Ultimately the diagnostic evaluation of alveolar hemorrhage usually includes bronchoscopic examination and bronchoalveolar lavage. Although nephrotic-range proteinuria may occur, full nephrotic syndrome is rarely seen. These antibodies are detected in approximately 95% of patients by immunoassays using various forms of purified or recombinant substrates. In those patients with pulmonary hemorrhage, clotting factors should be replaced by administering fresh-frozen plasma at the end of each treatment. Prednisone should be administered starting at a dose of 1 mg/kg of body weight for at least the first month and then tapered to alternate-day therapy during the second and third months of treatment. Cyclophosphamide is administered orally (at a dosage of 2 mg/kg/day, adjusted with consideration for the degree of impairment of kidney function and the white blood cell count) for 8 to 12 weeks. In a study at the Hammersmith Hospital in the United Kingdom, Gaskin and Pusey demonstrated that aggressive plasmapheresis, even in patients with severe renal insufficiency, may have an ameliorative effect and provide improved long-term patient and renal survival. All patients who required immediate dialysis and whose kidney biopsy specimens had crescents involving 100% of glomeruli remained dialysis dependent. Patients with a serum creatinine concentration higher than 7 mg/dL are unlikely to recover sufficient kidney function to discontinue renal replacement therapy. Aggressive immunosuppression and plasmapheresis are warranted in patients with pulmonary hemorrhage. Aggressive immunosuppression should be withheld in patients with disease limited to the kidney whose kidney biopsy specimens show widespread glomerular and interstitial scarring and who have a serum creatinine concentration of higher than 7 mg/dL at presentation. In patients who have an elevated serum creatinine level, yet whose biopsy specimens show active crescentic glomerulonephritis, aggressive treatment should continue for at least 4 weeks. If there is no restoration of kidney function without any evidence of pulmonary hemorrhage by 4 to 8 weeks, then, immunosuppression should be discontinued. The disease has a predilection for whites compared with blacks, and the prevalence of the disease is not significantly different in males compared with females (see Table 32. The periglomerular inflammation contains varying mixtures of neutrophils, eosinophils, lymphocytes, monocytes, and macrophages, including occasional multinucleated giant cells. This periglomerular inflammation area may have a granulomatous appearance, especially when the glomerulus that was the nidus of inflammation has been destroyed or is not in the plane of section. This granulomatous appearance is a result of the periglomerular reaction to extensive glomerular necrosis and is not specific for a particular category of necrotizing glomerulonephritis. Therefore, combinations of active acute necrotizing glomerular lesions and chronic sclerotic lesions often occur in the same kidney biopsy specimen. There is irregular staining for fibrin at sites of intraglomerular fibrinoid necrosis and capillary thrombosis and in the interstices of crescents. Foci of glomerular necrosis and sclerosis also may have irregular staining for C3 and IgM. On the other hand, the substantial accumulation of polymorphonuclear leukocytes at sites of vascular necrosis has led to examination of the role of neutrophil activation in this disease. In addition to the Fc receptormediated mechanism, substantial data support a role for the F(ab)2 portion of the antibody molecule in leukocyte activation. These results are corroborated by in vitro experiments demonstrating that blockade of the C5a receptor on human neutrophils abrogated their stimulation. Although yet to be confirmed, there is also preliminary evidence for this in humans, as abnormal levels of C3a, C5a, and soluble C5b-9 in plasma and urine have been identified in patients with active disease. Frequent sites of involvement are the eyes, ears, sinuses, upper airways, lungs, gastrointestinal tract, skin, peripheral nerves, joints, and central nervous system. However, some patients follow a more indolent course of slow decline in function and less active urine sediment. In the latter group of patients, episodes of focal necrosis and hematuria resolve with focal glomerular scarring. It is important to note that patients who have only pauciimmune crescentic glomerulonephritis at presentation may later develop signs and symptoms of systemic disease with involvement of extrarenal organ systems. Eight percent of patients died either from septic infections or from progressive recurrent vasculitis. The impact of kidney damage as a predictor of resistance emphasizes the importance of early diagnosis and prompt institution of therapy. Pauci-immune necrotizing glomerulonephritis and small vessel vasculitis may recur after kidney transplantation. Antigen-specific assays may be either enzyme-linked immunosorbent assays or radioimmunoassays. A variety of commercial tests are now available, and their diagnostic specificity ranges from 70% to 90%, and sensitivity from 81% to 91%.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.