
Kamagra Gold
General Information about Kamagra Gold
The dosage and frequency of the treatment may vary depending on the individual's response and health situation. It is important to observe the directions of the doctor and not exceed the beneficial dose. While Kamagra Gold has proven to be an efficient treatment for ED, it isn't a treatment. It is necessary to notice that it solely helps with the physical side of ED and doesn't address any underlying psychological or emotional causes. Therefore, it is crucial to consult a physician and handle any other contributing factors to ED. Like all drugs, Kamagra Gold may have side effects.
Kamagra Gold relaxes the graceful muscular tissues within the blood vessels of the penis, allowing for elevated blood move.
Some common unwanted facet effects include headache, dizziness, flushing, and indigestion. These unwanted facet effects are often mild and momentary, but if they persist or turn into bothersome, it's essential to inform a physician. There are additionally sure precautions and warnings to focus on before taking Kamagra Gold. It isn't really helpful for individuals with certain well being conditions similar to coronary heart disease, low blood pressure, or kidney and liver issues. It can be not really helpful to take with certain drugs, especially those that comprise nitrates, as it can result in a sudden drop in blood pressure.
Overall, Kamagra Gold could be a protected and effective option for men who're experiencing ED. It is essential to obtain the treatment from a good supply and observe the dosage and security pointers. Along with treatment, making way of life modifications corresponding to quitting smoking, maintaining a healthy weight, and managing stress can also improve ED symptoms. If ED persists or turns into a recurring problem, it's crucial to seek medical advice to ensure correct remedy and administration of the condition.
However, in males with ED, there's both not enough production of cGMP or an excessive amount of manufacturing of another enzyme that breaks it down. This leads to inadequate blood move to the penis, leading to difficulty in obtaining or sustaining an erection. Kamagra Gold works by inhibiting the enzyme that breaks down cGMP, allowing it to build up and have a longer-lasting effect. Kamagra Gold comes within the form of a pill and is typically taken orally. It is recommended to take it about half-hour to an hour earlier than sexual activity, and it might possibly last for about 4-6 hours.
In conclusion, ED is a typical condition that can have a major impact on a man's life. Kamagra Gold is a medication that works by rising blood circulate to the penis, permitting for higher erections. It is necessary to use this medicine responsibly and along side different way of life adjustments to successfully deal with ED and enhance general well-being.
In the presence of left ventricular outflow tract obstruction erectile dysfunction education kamagra gold 100 mg order overnight delivery, the arterial pulse has a rapid upstroke and downstroke (sometimes with a bisferiens character), the apex beat is sustained or double (reflecting a palpable atrial impulse followed by left ventricular contraction), and auscultation will demonstrate a systolic ejection murmur that is heard loudest at the left sternal edge and that radiates to the right upper sternal edge and apex (Chapter 51). Most patients with left ventricular outflow tract obstruction also have the murmur of mitral regurgitation, which results from failure of the mitral valve leaflets to coapt due to the systolic anterior motion of the mitral valve. In contrast, physical signs in most patients who do not have left ventricular outflow tract obstruction are subtle and are limited to features that reflect the hyperdynamic contraction (rapid upstroke pulse) and poorly compliant right (prominent a wave in jugular venous pressure) and left (S4 gallop, double-apex beat) ventricles (Chapter 51). The presence of predominantly distal or apical thickening is associated with giant negative T wave inversion, which is maximal in leads V3 and V4. Two-dimensional echocardiography (Chapter 55) is the mainstay of diagnostic imaging, but magnetic resonance imaging (Chapter 56) and computed tomography (Chapter 56) provide alternatives if the echocardiogram is of poor quality. In most patients, the hypertrophy is asymmetrical and involves the anterior and posterior intraventricular septum. The hypertrophy, however, may be more generalized and involve the free wall of the left ventricle, or it may be localized and confined to areas other than the septum, such as the lateral or posterior wall of the left ventricle. Patients with an outflow tract gradient of 30 mm Hg or more typically have systolic anterior motion of the mitral valve, with contact of either the anterior or (less commonly) the posterior mitral leaflet with the intraventricular septum during systole, in association with a posteriorly directed jet of mitral regurgitation, the severity of which is proportionate to the severity of the obstruction. Most patients with hypertrophic cardiomyopathy have left atrial enlargement as well as echocardiographic evidence of diastolic dysfunction. When it is available, cardiopulmonary exercise testing with metabolic gas exchange measurements provides an accurate and reproducible assessment of exercise capacity, which can be followed serially. Cardiac catheterization is rarely required for diagnosis or management, but it may be indicated when measurement of intracardiac pressures is required to guide therapeutic decisions. FamilyEvaluation DiagnosticCriteria A wall thickness of more than 2 standard deviations above the mean, corrected for age, gender, and height, is generally accepted as diagnostic. In the presence of other causes of left ventricular hypertrophy, such as long-standing systemic hypertension or aortic stenosis, the diagnosis of hypertrophic cardiomyopathy may be problematic. Such patients as well as those with chronically raised pulmonary pressures may requirediuretics. Disopyramide should be given concomitantly with a small to medium doseofa-blocker. Cardiac magnetic resonance images in a 70-year-old man with an electrocardiographic abnormality, previous ventricular tachycardia (nonsustained), and recentischemicstroke. Myocarditis Myocarditis, which is an inflammatory process involving the myocardium, can be caused by infections, immune-mediated damage, or toxins (Table 60-4). Worldwide, the most common infective myocarditis is Chagas disease, caused by Trypanosoma cruzi, a protozoan organism endemic in rural areas of South and Central America (Chapter 347). In the Western world, viral myocarditis is the most common cause of inflammatory heart disease. Smallpox vaccination (Chapter 18) causes myopericarditis with a reported incidence of 7. Other rare myocarditides include giant cell myocarditis, myocarditis complicating autoimmune disorders such as systemic lupus erythematosus (Chapter 266), and cocaine abuse (Chapter 34). Myocarditis is defined histologically by the presence of myocyte injury, with degeneration or necrosis, and an inflammatory infiltrate not due to ischemia. Initially, there is direct invasion of the myocardium by cardiotropic viruses, which enter the cardiomyocyte through receptor-mediated endocytosis. The viral genome, which translated intracellularly to produce viral protein or is incorporated into the host cell genome, may contribute to myocyte dysfunction by cleaving dystrophin. In the second phase, activation of the host immune system, including recruitment of natural killer cells and macrophages, increases the expression of proinflammatory cytokines such as interleukin-1 and tumor necrosis factor. This autoimmune response may result in long-term ventricular remodeling by direct effects on myocardial structural components or alterations in the extracellular matrix. Less common presentations include acute myocardial infarction with angiographically normal coronary arteries (Chapter 73), atrioventricular block (Chapter 64), and ventricular arrhythmias (Chapter 65). Patients with impairment of left ventricular function may present with symptoms and signs of fulminant cardiogenic shock (Chapter 107) with acute cardiovascular collapse. The diagnosis of myocarditis requires a high index of suspicion because it may mimic other common conditions. There are no typical features on echocardiography, but impaired left or right ventricular systolic performance (with or without ventricular dilation), regional wall motion abnormalities, left (or right) ventricular thrombus, diastolic impairment, and pericardial effusions may be present. Cardiac magnetic resonance imaging can detect myocardial inflammation and myocyte injury, with pericellular and cellular edema. Routine blood tests, such as full blood count and erythrocyte sedimentation rate, are usually unhelpful. Serum markers of myocardial injury, such as troponins T and I, may be elevated, but myocarditis may be proven by biopsy even in the absence of elevated serum troponin levels. Increased levels of autoantibodies against myocardial proteins (such as myosin and the adenine nucleotide translocator protein) are biomarkers of autoimmune myocarditis and correlate with progressive worsening of ventricular function. Cardiac magnetic resonance imaging with gadolinium enhancement can show evidence of myocarditis. In the United States, biopsy has generally been reserved for patients with heart failure refractory to standard management, features suggestive of systemic disease. By comparison, a European consensus statement recommends endomyocardial biopsy to achieve an etiologic diagnosis and to guide potential novel treatment options in patients with "clinically suspected myocarditis," 6 despite the absence of definitive outcome data to support this recommendation. When ventricular tachyarrhythmias or progressive heart failure are major features of clinically suspected myocarditis, particularly in a young person, endomyocardial biopsy is recommended to determine whether giant cell myocarditis is present.
In addition to injection erectile dysfunction effexor xr cheap kamagra gold on line, lidocaine can be administered topically as a gel or aerosol. Acute intoxication can occur, consisting of restlessness, anxiety, confusion, tachycardia, angina, cardiovascular collapse, convulsions, coma and death. In the central nervous system, initial stimulation gives rise to excitement and raised blood pressure followed by vomiting. It is most useful when a large total amount of local anaesthetic is needed or a high plasma concentration is likely. Compound benzocaine lozenges (containing 10 mg benzocaine) are used to alleviate the pain of local oral lesions, such as aphthous ulcers, lacerations and carcinoma of the mouth. Case history An 18-year-old white South African girl who had recently commenced the oral contraceptive was admitted with abdominal pain and proceeded to have a laparotomy. Anaesthesia was induced using thiopental and suxamethonium, and was maintained with isoflurane. Question What is the likely post-operative diagnosis and what may have precipitated this Answer Acute intermittent porphyria in association with: · · oral contraceptive pill; thiopental. Initial symptoms of overdose (excess local dose resulting in high plasma concentrations and systemic toxicity) may include light-headedness, sedation, circumoral paraesthesia and twitching. The total dose of lidocaine should not exceed 200 mg (or 500 mg if given in solutions containing adrenaline). Irrespective of the cause, its relief is one of the most important duties of a doctor. Fortunately, pain relief was one of the earliest triumphs of pharmacology, although clinicians have only recently started to use the therapeutic armamentarium that is now available adequately and rationally. Consequently, the intensity of pain is often poorly correlated with the intensity of the nociceptive stimulus, and many clinical states associated with pain are due to a derangement of the central processing such that a stimulus that is innocuous is perceived as painful. Trigeminal neuralgia is an example where a minimal mechanical stimulus triggers excruciating pain. The afferent nerve fibres involved in nociception consist of slowly conducting non-myelinated C-fibres that are activated by stimuli of various kinds (mechanical, thermal and chemical) and fine myelinated (A) fibres that conduct more rapidly but respond to similar stimuli. The gate provided by the substantia gelatinosa can also be activated centrally by descending pathways. The main pathway from this area runs to the nucleus raphe magnus in the medulla and thence back to the dorsal horn of the cord connecting with the interneurones involved in nociception. Stimulation of nociceptive endings in the periphery is predominantly chemically mediated. Capsaicin, the active principle of red peppers, potently stimulates and then desensitizes nociceptors. Pain differs from nociception because of central mechanisms, including an emotional component. It has no irritant effect on the gastric mucosa and can be used safely and effectively in most individuals who are intolerant of aspirin. Mechanism of action Paracetamol inhibits prostaglandin biosynthesis under some circumstances. There is no convincing evidence that paracetamol causes chronic liver disease when used regularly in therapeutic doses (4 g/24 hours). Paracetamol is structurally closely related to phenacetin (now withdrawn because of its association with analgesic nephropathy) raising the question of whether long-term abuse of paracetamol also causes analgesic nephropathy, an issue which is as yet unresolved. Pharmacokinetics, metabolism and interactions Absorption of paracetamol following oral administration is increased by metoclopramide, and there is a significant relationship between gastric emptying and absorption. The major sulphate and glucuronide conjugates (which account for approximately 95% of a paracetamol dose) are excreted in the urine. However, unlike paracetamol it also has antiinflammatory properties when used in high doses. Various preparations are available, including regular as well as buffered, soluble and enteric-coated forms. Enteric coating is intended to reduce local gastric irritation, but much of the gastric toxicity is due to inhibition of gastric mucosal prostaglandin biosynthesis (see below), rather than to direct gastric irritation. Consequently, slow-release preparations do not eliminate the adverse effects of aspirin on the gastric mucosa. In addition, aspirin and similar drugs can directly activate eosinophils and mast cells in these patients through IgE-independent mechanisms. Some of the selectivity of aspirin for platelet cyclo-oxygenase is probably due to exposure of platelets to high concentrations of aspirin in portal blood, whereas tissues are exposed to the lower concentrations present in the systemic circulation. Salicylate is metabolized in the liver by five main parallel pathways, two of which are saturable (MichaelisMenten kinetics) and is also excreted unchanged in the urine by a first-order process. Michaelis-Menten Salicyl phenolic glucuronide (20%) salicylate has dose-dependent (non-linear) kinetics (Chapter 3) at high therapeutic doses or after overdose. Urinary elimination of salicylate is considerably influenced by pH, being more rapid in alkaline urine, which favours the charged (polar) anionic form that is not reabsorbed, rather than the free acid (Chapter 6). This property is utilized in the treatment of salicylate overdose by urine alkalinization and demonstrates the principle of ion trapping. They occasionally cause local irritation of the skin, but adverse effects are otherwise uncommon. It is less of a respiratory depressant than the opioids and does not cause dependence. Drug interactions Aspirin increases the risk of bleeding in patients receiving anticoagulants via effects on platelets, gastrotoxicity and, in overdose, by a hypoprothrombinaemic effect. Aspirin should not be given to neonates with hyperbilirubinaemia because of the risk of kernicterus as a result of displacement of bilirubin from its binding site on plasma albumin (Chapter 13). It reduces the efficacy of antihypertensive medication and of diuretics by blocking formation of vasodilator and natriuretic prostaglandins in the kidney.
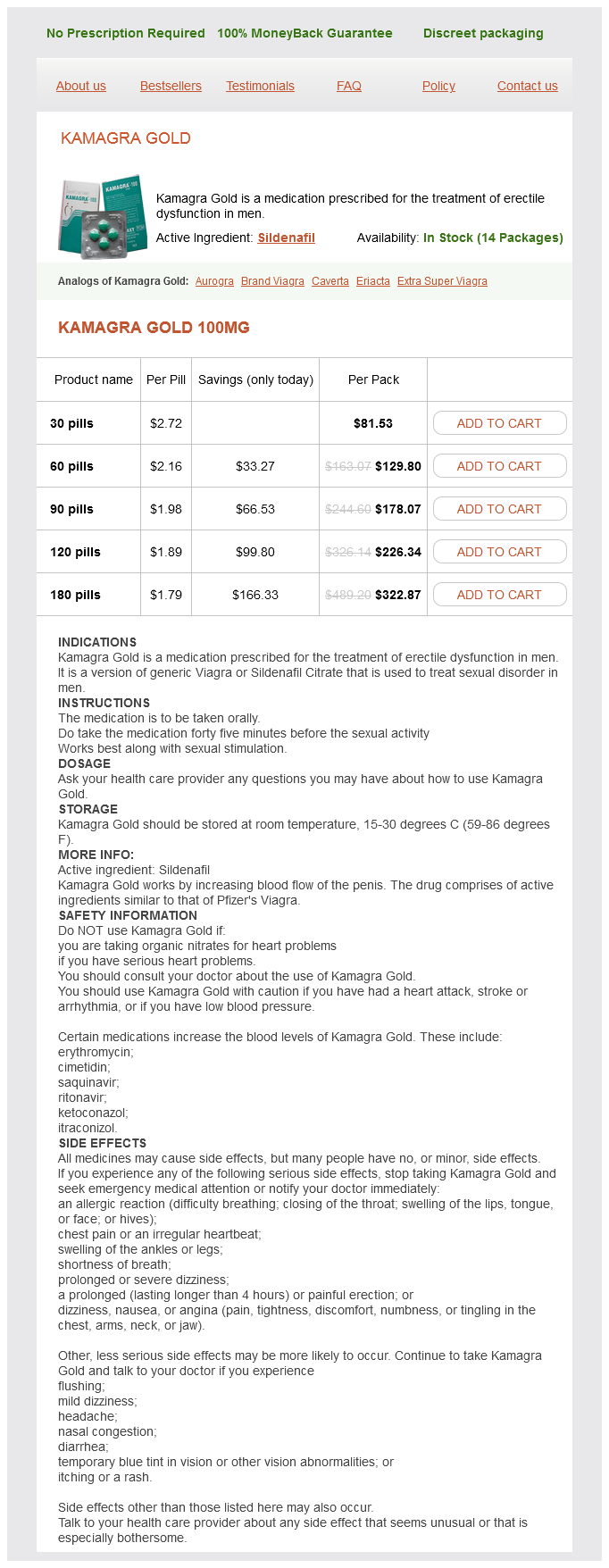
Kamagra Gold Dosage and Price
Kamagra Gold 100mg
- 30 pills - $81.53
- 60 pills - $129.80
- 90 pills - $178.07
- 120 pills - $226.34
- 180 pills - $322.87
Despite recovery from an acute attack erectile dysfunction fatigue order 100 mg kamagra gold with mastercard, patients are at greatly increased risk of death or serious illness from intercurrent respiratory infections, and administration of influenza and pneumococcal vaccines is important. Airways obstruction is invariably present in chronic bronchitis, but is of variable severity. In some patients there is a reversible element, and a formal trial of bronchodilators, either 2-adrenoceptor agonists or anticholinergics. Many patients are not steroid responsive; approaches designed to reverse glucocorticosteroid resistance, including theophylline, are currently under investigation. The mortality of such patients is related to pulmonary hypertension, which is increased by chronic hypoxia. Relief of hypoxia on a long-term basis by increasing the concentration of inspired oxygen reverses the vasoconstriction in the pulmonary arteries and decreases pulmonary hypertension. Long-term oxygen therapy cannot be safely offered to patients who continue to smoke because of the hazards of fire and explosion. For asthma, 2-agonists are given via inhalation where possible, see also Table 33. Some patients are unable to master this technique; · aerosol administered via a nebulizer; · as a dry powder almost all patients can use a drypowder inhaler correctly. Most (approximately 90%) of the dose administered by aerosol is swallowed, but the 1015% which is inhaled largely remains as free drug in the airways. Salmeterol is long acting, with a duration of action of at least 12 hours, allowing twice daily administration. The lipophilic side-chain of salmeterol binds firmly to an exo-site that is adjacent to , but distinct from, the 2-agonist binding site. The degree and rate of onset of bronchodilatation are less than those of salbutamol, but the duration of response is longer. Ipratropium has a place in maintenance therapy and the treatment of acute severe attacks of asthma and chronic bronchitis. Side effects include gastro-intestinal disturbances, vasodilatation, dysrhythmias, seizures and sleep disturbance. Mechanism of action There is increased parasympathetic activity in patients with reversible airways obstruction, resulting in bronchoconstriction through the effects of acetylcholine on the muscarinic (M2, M3) receptors in the bronchi. Oral theophylline may be used for less severe symptoms or to reduce nocturnal asthma symptoms. Recently, the use of theophylline has markedly declined, but it is still sometimes used in refractory cases. For intravenous aminophylline, a loading dose given slowly (2030 minutes) is followed by a maintenance infusion. Oral theophylline sustained-release preparations can provide effective therapeutic concentrations for up to 12 hours following a single dose. Because of their slow release rate they have a reduced incidence of gastro-intestinal side effects. Adverse effects these include: · bitter taste (this may compromise compliance); · acute urinary retention (in patients with prostatic hypertrophy); · acute glaucoma has been precipitated when nebulized doses are given via a face mask; · paradoxical bronchoconstriction due to sensitivity to benzalkonium chloride, which is the preservative in the nebulizer solution. Mechanism of action and pharmacological effects It is not clear exactly how theophylline produces bronchodilation. Its pharmacological actions include the following: · relaxation of airway smooth muscle and inhibition of mediator release. Pharmacokinetics When administered by aerosol, it is poorly absorbed systemically. Plasma t1/2 is three to four hours and inactive metabolites are excreted in the urine. Several formulations of 2-agonist combined with muscarinic antagonist bronchodilators are available to simplify treatment regimens. Anticholinergics · Antagonist at M2 and M3 muscarinic receptors in the bronchi, causing bronchodilatation. Adverse effects the adverse effects of theophylline are: · Gastro-intestinal: nausea, vomiting, anorexia. The therapeutic concentration range is 520 mg/L, but it is preferable not to exceed 10 mg/L in children. They are used both in maintenance therapy (prophylaxis) and in the treatment of the acute severe attack. This delay is due to the action of glucocorticosteroids via altered gene transcription and subsequent modified protein synthesis. Its use as a prophylactic in children has been largely superseded by inhaled glucocorticosteroids which are more effective. It is used as a nasal spray for perennial and allergic rhin-itis, and as eyedrops in allergic conjunctivitis. Mechanism of action Cromoglicate and nedocromil inhibit mediator release from sensitized mast cells in vitro, and also reduce firing of sensory Key points Anti-inflammatory agents cromoglicate and glucocorticosteroids Sodium cromoglicate · · · · · · Its mechanism of action is unclear. Use Modern inhalational devices deliver up to 20% of the administered dose to the lungs. The fluorinated derivatives are extremely potent and mainly exert a local action because they are highly polar and hence only a small fraction of the dose is systemically absorbed. The comparative pharmacology of the commonly used inhaled glucocorticosteroids is summarized in Table 33. May be used in children to avoid systemic steroids Fluticasone 18 1200 May cause fewer systemic side effects than others a Relative to dexamethasone binding to glucocorticosteroid receptors in vitro and blanching of human skin in vitro. However, the complete mechanism underlying their therapeutic efficacy is uncertain. Use Leukotriene receptor antagonists are used to treat asthma and are given orally, usually in the evening.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.