
Kamagra Oral Jelly
General Information about Kamagra Oral Jelly
One of the principle explanation why Kamagra Oral Jelly has gained recognition is its decrease cost. As a generic medicine, it is considerably cheaper than Viagra, making it a extra inexpensive choice for those in search of ED remedy. This accessibility has made it particularly popular in nations where Viagra just isn't readily available or is too costly.
While Kamagra Oral Jelly could have many benefits, it's essential to notice that like another medicine, it does have potential side effects. These can include headaches, dizziness, flushing, and indigestion. It can additionally be not beneficial for these with heart situations or taking medication for high blood pressure. As with any medication, it is important to consult with a health care provider before starting remedy.
Kamagra Oral Jelly is available in various strengths of 100mg, just like Viagra. It is really helpful to take the medication about 30-45 minutes before sexual exercise, and the effects can last up to 4-6 hours. Like all drugs, it is essential to follow the recommended dosage and not exceed the prescribed quantity as it can lead to opposed results.
Erectile dysfunction (ED) is a common situation that impacts tens of millions of men worldwide. It is defined as the lack to achieve or maintain an erection sufficient for sexual activity. Although there are many treatment options out there for this situation, Kamagra Oral Jelly presents a unique and handy solution that has gained popularity amongst ED victims.
Kamagra Oral Jelly is a product of Ajanta Pharma, an Indian pharmaceutical firm that specializes in producing generic medicines. This jelly resolution accommodates the energetic ingredient sildenafil citrate, the same ingredient discovered in the well-liked erectile dysfunction treatment Viagra. However, Kamagra Oral Jelly is not only a generic form of Viagra, it is obtainable in a special kind that units it aside from conventional pills and tablets – a flavored jelly.
But the most vital advantage of Kamagra Oral Jelly is its quicker onset of action. As it's in a liquid type, the lively ingredient is quickly absorbed into the bloodstream, resulting in a quicker response time. This means that males can achieve an erection in a shorter amount of time, making it a super choice for these in search of a spontaneous and discreet answer to their ED.
The use of a jelly formulation could appear uncommon for an erectile dysfunction remedy, however it has some advantages over conventional pills. The first being that it's easier to swallow, particularly for those who have problem swallowing tablets. It additionally has a extra nice taste, making it a more pleasant expertise for customers.
In conclusion, Kamagra Oral Jelly is a singular and handy resolution for the therapy of erectile dysfunction. It provides a sooner onset of action, easier administration, and lower value in comparability with traditional tablets, making it a preferred choice amongst ED sufferers. However, it's important to make use of it responsibly and seek the guidance of with a doctor earlier than starting remedy. With proper use and underneath medical supervision, Kamagra Oral Jelly may help men regain their confidence and improve their sexual perform.
Primary localized amyloidosis of the urinary bladder: a case series of 31 patients erectile dysfunction 23 discount 100 mg kamagra oral jelly visa. Inflammatory pseudotumor of the urinary bladder-possible relationship to nodular fasciitis. A clinicopathological, immunohistochemical, ultrastructural, and flow cytometric study of 13 cases. Inflammatory pseudotumor of the urinary bladder: a report of five cases and review of the literature. Inflammatory pseudotumor of the urinary bladder with aberrant expression of cytokeratin. Clinical utility of immunohistochemistry in the diagnoses of urinary bladder neoplasia. Inflammatory myofibroblastic tumors of the genitourinary tract-single entity or continuum Ureteral endometriosis: clinicopathological and immunohistochemical study of 7 cases. Endometriosis of the urinary tract: a review of the literature and a report of four cases of vesical endometriosis. Malignant transformation in endometriosis of the urinary bladder: case report of clear cell adenocarcinoma. Immunohistochemical phenotype of the urinary bladder endocervicosis: comparison with normal endocervix and well-differentiated mucinous adenocarcinoma of uterine cervix. An attempt towards a systematic account of the appearances connected with that malconformation of the urinary organs in which the ureters, instead of terminating in a perfect bladder, open externally on the surface of the abdomen. Adenocarcinoma arising in exstrophy of the bladder: report of two cases and review of the literature. The obstetric and gynaecological complications of bladder exstrophy and epispadias. The importance of a successful initial bladder closure in the surgical management of classical bladder exstrophy: analysis of 144 patients treated at the Johns Hopkins Hospital between 1975 and 1985. Double bladder and related anomalies: clinical and embryological aspects and a case report. Incomplete reduplication of the bladder with congenital solitary kidney; report of a case. Congenital deficiency of the abdominal musculature and associated genitourinary anomalies: a report of 22 cases. Embryology, anatomy, and diseases of the umbilicus together with diseases of the urachus. Diverticulum of the bladder- presentation and evaluation of treatment of 115 cases. The spectrum of histopathologic findings in vesical diverticulum: implications for pathogenesis and staging. Congenital bladder diverticulum presenting as bladder outlet obstruction in infants and children. Limited smoothelin expression within the muscularis mucosae: validation in bladder diverticula. Primary carcinoma in a diverticulum of the bladder, a report of four cases and review of the literature. Primary osteosarcoma of bladder diverticulum mimicking intradiverticular calculus: a case report. The superficial cells are often prominent and may have vacuolization of the cytoplasm, eosinophilic syncytial or apocrine-like morphology, or may demonstrate mucinous metaplasia. Secondary budding of small fronds from larger simple primary papillary fronds is commonly observed. Inverted Papilloma Inverted papilloma is usually found in males in the sixth or seventh decade of life. Although the term inverted papilloma was initially introduced in 1963 by Potts and Hirst to describe this architecturally distinctive urothelial neoplasm, the Viennese urologist Paschkis had previously reported four morphologically identical urothelial tumors in 1927 under the name of adenomatoid polyp. These invaginating structures demonstrate mature urothelium centrally, with darker and palisading basal cells peripherally, usually surrounded by fibrotic stroma without marked inflammation. The glandular variant is composed of nests of urothelium with either pseudoglandular spaces lined by mature urothelium or even true glandular elements, containing mucicarminophilic secretions and mucous-secreting cells. The glandular variant, as proposed by these investigators, has considerable morphologic overlap with florid cystitis glandularis and is not widely accepted as a diagnostic entity. Within the spectrum of findings in inverted papilloma, vacuolization and foamy xanthomatous cytoplasmic changes may be seen. These "clear cells" may be concentrated within distinct regions of the tumor, but more frequently are diffusely intermingled with usual inverted papilloma cells. Foci of nonkeratinizing squamous metaplasia and neuroendocrine differentiation have been reported. Some cases may demonstrate focal minor cytologic atypia that is likely degenerative in nature and has no clinical significance. Such distinction may be difficult, especially in limited biopsy specimens or when interpretation is confounded by crush artifact. In contrast, urothelial carcinoma with an inverted growth pattern often has thick and irregular tumor columns with transition to more solid nests.
Note the beveled tibia and the proximal shortening of the fibula compared with the tibia erectile dysfunction protocol scam alert purchase genuine kamagra oral jelly online. Generally drains are, not necessary in below-knee amputations for peripheral vascular disease; however, drains are frequently used in below-knee amputations performed for trauma or other reasons. If a drain is required, I prefer a closed suction drain, which is brought through a separate stab wound in the lateral aspect of the lower leg. The sural nerve (posterior flap) is identified, pulled down, ligated, transected, and allowed to retract back from the edge of the flap. The flap is rotated anteriorly and the muscle fascia of the posterior flap is, approximated to the anterior fascia with interrupted absorbable sutures. The skin is carefully approximated with interrupted vertical mattress sutures using a monofilament plastic or metal suture. I avoid the use of tissue forceps and believe that closure of the below-knee stump, especially in patients with peripheral vascular disease, should be performed with the care of a plastic surgical procedure. Tailoring the corner of the skin flap may be required to prevent excessive dog ears. The use of a rigid plaster of Paris dressing incorporating the knee is ideal, regardless of whether an immediate postoperative prosthesis will be used. A rigid dressing controls edema, promotes healing, and protects the stump during the postoperative period. Application of an immediate postoperative prosthesis as part of the rigid dressing is described in detail later. Advantages and Disadvantages the below-knee amputation is an extremely durable amputation. The likelihood of primary healing is very good, and the ability to rehabilitate a patient with a below-knee prosthesis is excellent. In a report by Kim and coworkers in 1976, 90% of their patients with unilateral below-knee amputations were able to ambulate. Prosthetic Requirements and Rehabilitation Potential A below-knee prosthesis is required for ambulation at this level of amputation. A variety of prostheses are available, but all generally involve total stump contact (with or without a prosthesis liner) with weight bearing on the patellar tendon and tibial-fibular condyles. Newer types of below-knee prostheses incorporate total contact and total weight-bearing designs. These prostheses can incorporate a variety of feet, some of which have flexion and extension motion or "ankle rotation" (with weight loading) or energy storage (Seattle Foot [Model & Instrument Works, Inc. The energy requirement for a unilateral below-knee amputee is increased approximately 40% to 60% compared with normal (energy consumption with an energy-storing leg has not yet been reported). It has been my experience, as well as that of others, that any patient (regardless of age) who was ambulatory before below-knee amputation and who undergoes amputation within 30 days of hospital entrance can ambulate successfully on a below-knee prosthesis. In fact, most patients who require bilateral below-knee amputations can ambulate successfully as shown by Roon and associates. The time required for gait training for a unilateral belowknee amputee is approximately 2 to 3 weeks, and most patients develop a very good gait pattern. There are some physical limitations for geriatric below-knee amputees; however, young below-knee amputees are able to negotiate ladders, stairs, and other obstacles with minimal difficulty. Knee Disarticulation Indications the indications for knee disarticulation amputation are limited, and it is performed primarily on young, active males for whom the advantages of strength and serviceability outweigh prosthetic cosmesis. Disarticulation amputation of the knee is the second most technically difficult lower extremity amputation following Syme amputation. Successful performance of a knee disarticulation amputation with a high degree of primary healing usually requires some type of objective technique of preoperative amputation level selection. Knee disarticulation is indicated primarily when the gangrenous process, infection, trauma, tumor, or orthopedic disability encroaches too close to the anterior and posterior (or sagittal) limits of a below-knee amputation flap or has resulted in an unsalvageable knee joint. Another potential indication for knee disarticulation is a patient who has had either acute or chronic failure of a below-knee amputation in whom skin flaps at the knee are viable enough to consider knee disarticulation. In general, British surgeons have been more enamored of knee disarticulation than their American colleagues. Interest in this level of amputation has arisen as a result of advances in cosmetic prosthetic components and prosthetic fitting techniques. Moreover, in a study of 169 unilateral lower extremity amputees, Houghton and coworkers found that rehabilitation results were better for through-knee amputation (62%) than for aboveknee (33%) (P <. Surgical Technique There are two excellent reviews of the surgical techniques of disarticulation of the knee111,112; therefore they are described only briefly here. I prefer the knee disarticulation technique described by Burgess,111 owing to failure with other types of knee disarticulation amputation and success using the modified Burgess technique. Anesthetic management of knee disarticulation is best handled with either spinal or general anesthesia, with the patient in the prone position. The operation can be performed, but is more difficult, with the patient in the supine position. At the discretion of the surgeon, a gown or pack can be placed beneath the thigh to hyperextend the hip joint and provide an easier working surface on the anterior portion of the knee and lower leg. A marking pencil should be used to outline the skin flaps before making the skin incision. Construction of the knee disarticulation skin flaps is crucial to avoid tension on the skin suture line when the amputation stump is closed. Dissection is first carried anteriorly down to the insertion of the patellar tendon on the tibia. The tendon is severed at its insertion and sharply dissected proximally Deep dissection on the medial side of the. On the lateral side of the knee, the tendon of the biceps femoris muscle and iliotibial band are sectioned low.
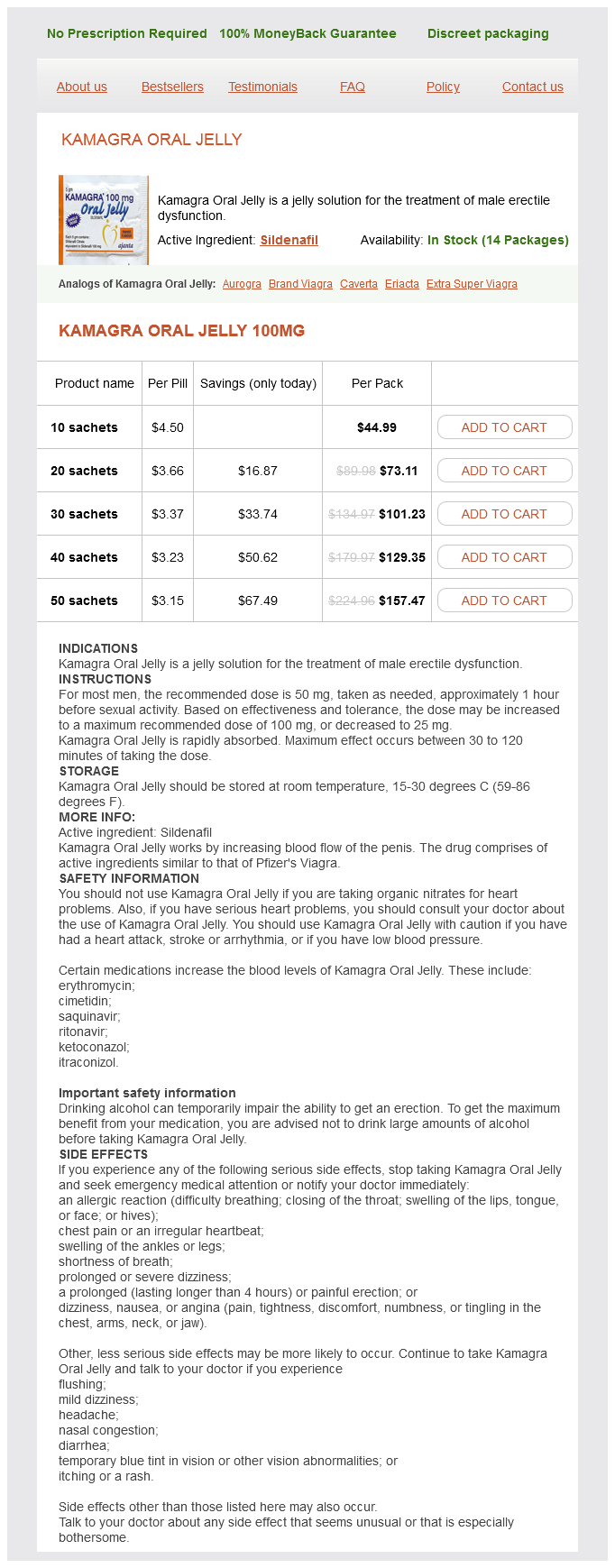
Kamagra Oral Jelly Dosage and Price
Kamagra Oral Jelly 100mg
- 10 sachets - $44.99
- 20 sachets - $73.11
- 30 sachets - $101.23
- 40 sachets - $129.35
- 50 sachets - $157.47
Prostatic carcinoma with signet ring cells: a clinicopathologic and immunohistochemical analysis of 12 cases erectile dysfunction treatment injection therapy kamagra oral jelly 100 mg lowest price, with review of the literature. Primary signet ring cell adenocarcinoma of the prostate treated by radical prostatectomy after preoperative androgen deprivation. Locally-confined signetring cell carcinoma of the prostate: a case report of a long-term survivor. Prostate cancer presenting with malignant ascites: signet-ring cell variant of prostatic adenocarcinoma. Exaggerated signet-ring cell change in stromal nodule of prostate: a pseudoneoplastic proliferation. Immunoperoxidase localization of prostatic acid phosphatase in prostatic carcinoma with sarcomatoid changes. Histologic variants of adenocarcinoma and other carcinomas of prostate: pathologic criteria and clinical significance. Sarcomatoid carcinoma of the prostate: progression from adenocarcinoma is associated with p53 over-expression. Prostate cancer progression in the presence of undetectable or low serum prostate-specific antigen level. Carcinosarcoma of the prostate: two cases with distinctive morphologic and immunohistochemical findings. Adenocarcinoma arising from the prostatic duct mimicking transitional cell carcinoma. Ductal adenocarcinoma of the prostate diagnosed on needle biopsy: correlation with clinical and radical prostatectomy findings and progression. Ductal carcinomas of the prostate: a clinicopathological and immunohistochemical study. Ductal (endometrioid) adenocarcinoma of the prostate: a clinicopathological study of 16 cases. Metastatic ductal adenocarcinoma of the prostate: cytologic features and clinical findings. Prognostic significance of the proportion of ductal component in ductal adenocarcinoma of the prostate. Distribution pattern of basal cells detected by cytokeratin 34 beta E12 in primary prostatic duct adenocarcinoma. High-grade prostatic intraepithelial neoplasialike ductal adenocarcinoma of the prostate: a clinicopathologic study of 28 cases. Macrocystic ductal adenocarcinoma of prostate: a rare gross appearance of prostate cancer. Spectrum of cystic epithelial tumors of the prostate: most cystadenocarcinomas are ductal type with intracystic papillary pattern. Immunohistochemistry of ductal adenocarcinoma of the prostate and adenocarcinomas of non-prostatic origin: a comparative study. Endometrioid adenocarcinoma of the prostate: a clinicopathologic and immunohistochemical study. Ductal adenocarcinoma of the prostate: histogenesis, biology and clinicopathological features. Clinicopathological features of prostate ductal carcinoma: matching analysis and comparison with prostate acinar carcinoma. Contemporary populationbased comparison of localized ductal adenocarcinoma and high-risk acinar adenocarcinoma of the prostate. Prostatic duct adenocarcinoma with endometrioid features: immunohistochemical and electron microscopic study. Historical and contemporary perspectives on cribriform morphology in prostate cancer. Presence of invasive cribriform or intraductal growth at biopsy outperforms percentage grade 4 in predicting outcome of Gleason score 3 + 4 ¼ 7 prostate cancer. Prostatic comedocarcinoma: correlation of sonograms with pathologic specimens in three cases. Flow cytometric analysis of comedocarcinoma of the prostate: an uncommon histopathological variant of prostatic adenocarcinoma. Neuroendocrine differentiation and markers of cell proliferation in a group of patients with prostate adenocarcinoma and normal or high serum prostate-specific antigen levels. Prognostic significance of neuroendocrine expression in lymph node-positive prostate cancer. Immunohistochemical and ultrastructural features of neuroendocrine differentiated carcinomas of the prostate: an immunoelectron microscopic study. Fixemer T [Neuroendocrine differentiation in prostate cancer: an unrecognized and therapy resistant phenotype]. Neuroendocrine differentiation in hormone refractory prostate cancer following androgen deprivation therapy. Neuroendocrine differentiation in human prostate tissue: is it detectable and treatable Prostate carcinoma with neuroendocrine differentiation: case report and literature review. Relationship between neuroendocrine features and prognostic parameters in human prostate adenocarcinoma. Neuroendocrine differentiation and short-term neoadjuvant hormonal treatment of prostatic carcinoma with special regard to tumor regression.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.