
Levitra Professional
General Information about Levitra Professional
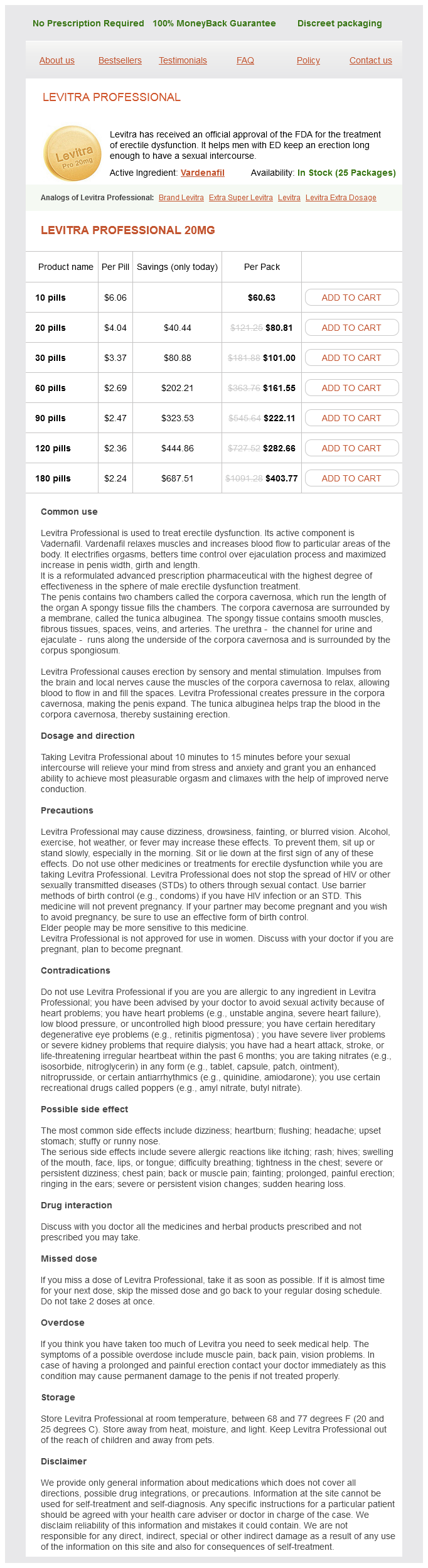
Approved by the FDA in 2018, Levitra Professional incorporates a better focus of vardenafil, making it a more potent medication. This signifies that it could provide longer-lasting and stronger erections, making it a most well-liked alternative for many men that suffer from ED. In reality, a clinical trial confirmed that sufferers taking Levitra Professional skilled significant improvement in their ability to achieve and maintain an erection compared to these taking the standard model of the medicine.
Another good thing about Levitra Professional is its safety profile. As with any treatment, there may be some unwanted facet effects, but they are usually delicate and temporary. The most commonly reported unwanted effects with Levitra Professional embody headache, flushing, and nasal congestion. However, these signs usually are not severe and normally subside on their own with none medical intervention. Moreover, the protection and efficacy of Levitra Professional have been evaluated and permitted by the FDA, giving sufferers the reassurance that they're utilizing a trusted and dependable medicine.
One essential issue to consider whereas choosing an ED treatment is its compatibility with other medications. This is the place Levitra Professional stands out from its competitors. It has a low likelihood of interacting with other medicines, making it an appropriate selection for patients who're on other forms of treatment. However, it is essential to disclose any drugs you are at present taking to your physician before starting Levitra Professional to make sure its secure use.
Levitra Professional is a new and improved version of the original Levitra, which has been on the market for nearly two decades. The commonplace model of Levitra contains vardenafil, a PDE5 inhibitor, which works by enjoyable the muscle tissue and growing blood flow to the penis, thus aiding in reaching and maintaining an erection. However, with Levitra Professional, the formulation has been enhanced to offer an much more efficient remedy for ED.
In today’s fast-paced world, it’s easy to miss the significance of sexual well being. However, for many men, maintaining a wholesome sex life can greatly impact their general well-being and relationships. Unfortunately, erectile dysfunction (ED) is a common problem that may greatly have an result on a man’s capability to carry out sexually. Thankfully, there are medicines out there that may help alleviate this drawback. One such medication is Levitra Professional, which has recently gained official approval from the Food and Drug Administration (FDA) for the remedy of erectile dysfunction.
In today’s digital era, every little thing is out there at our fingertips, and so is Levitra Professional. With a sound prescription, one can conveniently buy this treatment on-line from respected on-line pharmacies. This saves patients the trouble and discomfort of discussing their situation with a pharmacist in person. However, it's crucial to choose a respectable and reliable on-line pharmacy to make sure the authenticity and high quality of the medicine obtained.
One of the main causes for the recognition of Levitra Professional is its fast-acting nature. It has been reported to work in as little as quarter-hour, making it the fastest-acting ED medicine in the marketplace. This is a major benefit for men who want to be spontaneous with their sexual activity, as they not need to plan their intimate moments round medication timings. This also means that men can enjoy more flexibility of their sexual relationships with none worrying in regards to the timing of medicine.
In conclusion, with the official approval from the FDA, Levitra Professional has solidified its place as a potent and reliable treatment for ED. Its enhanced formulation, sooner onset of motion, and minimal unwanted effects make it a preferred treatment for a lot of males dealing with ED. However, it is important to seek the assistance of with a healthcare professional earlier than utilizing this or some other ED medication. With correct steering and the best medicine, men can take management of their sexual well being and enjoy a satisfying intercourse life.
There is insufficient evidence to support the use of pelvic nerve interruption for the relief of primary or secondary dysmenorrhoea [A] herbal erectile dysfunction pills canada purchase levitra professional with a visa. There is no evidence that division of adhesions relieves chronic pelvic pain, with the possible exception of severe dense avascular adhesions [B]. Where possible, chronic pelvic pain should be managed in a multidisciplinary clinic [A]. Primary dysmenorrhoea is experienced by more than two thirds of women and a minority are severely incapacitated. Investigation of suspected primary dysmenorrhoea is unnecessary unless there are atypical symptoms or abnormal findings on pelvic examination [C]. The multifactorial nature of chronic pelvic pain should be discussed and explored from the start [B]. Pain resulting from disturbances in the central or peripheral nervous system (neuropathic pain) is an important component of chronic pelvic pain [C]. Alternative therapies, including physical and behavioural therapy, dietary supplements (magnesium, vitamin B1) and References 1. The prevalence of chronic pelvic pain in women in the United Kingdom: a systematic review. Prevalence and incidence of chronic pelvic pain in primary care: evidence from a national general practice database. Chronic pelvic pain: prevalence, healthrelated quality of life and economic correlates. Optimum management of chronic cyclical pelvic pain: an evidence-based and pragmatic approach. Changes in regional gray matter volume in women with chronic pelvic pain: a voxel-based morphology study. A systematic review of the accuracy of ultrasound in the diagnosis of endometriosis. A randomized clinical trial to compare two different approaches in women with chronic pelvic pain. Continuous compared with cyclic oral contraceptives for the treatment of primary dysmenorrhoea: a randomized controlled trial. The effects of an oestrogen-free, desogestrel-containing oral contraceptive in women with cyclical symptoms: results from two studies on oestrogen-related symptoms and dysmenorrhoea. A randomized controlled trial of medroxyprogesterone acetate and psychotherapy for the treatment of pelvic congestion. Randomized controlled trial of depot leuprolide in patients with chronic pelvic pain and clinically suspected endometriosis. Antidepressant-induced analgesia in chronic non-malignant pain: a meta-analysis of 39 placebo-controlled studies. Laparoscopic adhesiolysis in patients with chronic abdominal pain: a double blind randomised controlled multicentre trial. This is considerably lower than previous estimates based on series of women undergoing laparoscopy for various indications. In a prospective study of 1542 Caucasian women in a single Scottish centre2 endometriosis was visualised in 6 per cent of women undergoing sterilisation, 21 per cent being investigated for infertility and 15 per cent being investigated for pelvic pain. Prevalence in other case series of women undergoing laparoscopy for investigation of pelvic pain has generally been higher, varying between 23 and 80 per cent. It is most typically diagnosed in women aged 2530 years but has been described in adolescents, in particular those with structural abnormalities of the reproductive tract. Factors which reduce menstruation, such as pregnancy and the use of oral contraceptives,24 reduce its prevalence while early menarche, shorter menstrual cycles and nulliparity are associated with increased prevalence. There are no clear racial or ethnic differences but the incidence is increased 710-fold among firstdegree relatives. It is a common condition with many diverse manifestations and a clinical course that is highly variable and unpredictable. It may be asymptomatic, but most commonly presents with pelvic pain that is typically cyclical and in severe cases there may be associated bowel or bladder symptoms. The site of the lesions deep in the pelvis can also cause dyspareunia and there is a well-recognised but poorly understood association with subfertility. Endometriosis is usually regarded as distinct from adenomyosis (see Chapter 78), in which endometrial tissue is present within the myometrium. This chapter deals mainly with the management of pain in endometriosis, which has attracted a large literature and for which evidence-based management is relatively well developed. Haematogenous or lymphatic spread in a minority of cases may account for the rare occurrence of endometriosis at distant sites. Retrograde menstruation is observed in up to 90 per cent of women but only a minority of women develop endometriosis. It is most likely that tissue implantation is a result of failure of clearance mechanisms which may be secondary to defects in the local peritoneal immune defence system in susceptible individuals. Whatever the underlying mechanisms, it is evident that the symptoms and the progression of the disease differ considerably amongst individuals, with a poor correlation between laparoscopic appearances and clinical symptoms. Results from second-look laparoscopy in treatment trials3 have found short-term spontaneous regression of lesions in around one third of women receiving no active treatment, no change in another third and progression in the remaining third. Genetic factors appear to be relevant and these may influence local response mechanisms and the subsequent course of the disease. Endometriomas, also known as chocolate cysts, are retention cysts which form when inflammatory adhesions develop between endometriotic deposits on the ovary and the pelvic side wall or around a superficial ovarian lesion, producing progressive inversion of the surrounding cortex. Endometriomas may be multiple and very large, when they inevitably interfere with fertility by adhesion and distortion of the Fallopian tubes. In some women with endometriotic lesions predominantly affecting the uterosacral ligaments, marked fibrosis and scarring may develop, with infiltration of active endometriotic tissue into the rectovaginal septum or laterally to involve the ureters.
Often a child will be subjected to more than one type of abuse erectile dysfunction drugs market discount levitra professional 20 mg fast delivery, highlighting the need to undertake a holistic assessment of the child. Therefore much of the risk for children will be determined by who their carers are and who has access to them. Over 90 per cent of children who experienced sexual abuse were abused by someone they knew. More than one in three children (34 per cent) who experienced contact sexual abuse by an adult did not tell anyone else about it. Where abuse is suspected it is important that there is an opportunity for the child to disclose what is happening, bearing in mind that the child may be reluctant to provide details within earshot of carers in attendance. In addition a child may have been manipulated or threatened by the abuser not to tell. Key messages for the generalist would be to have a high level of suspicion and to involve senior colleagues at an early stage. In addition, the arrival of new technologies has seen the development of new practices such as online grooming and abuse, sexting, etc. Child sexual exploitation is something that will have been happening throughout the centuries and yet is only now beginning to be recognised. Recent inquiries have shown that these children were often failed by professionals, who had been judgemental in their assessment of the behaviour and circumstances of the children and had failed to pick up on the signs and symptoms of sexual abuse. Any examination should be preceded by a careful discussion with the child and/or carer that covers issues around consent for the examination, the limitations of confidentiality, disclosure of information for safeguarding purposes, etc. Given that sexual abuse is about the disregard of consent and the abuse of power, great care must be taken by healthcare workers not to repeat this process. Careful consideration must be given by the doctor to balance what may sometimes seem to be competing pressures, such as the child requesting information regarding sexual activity not be shared, the need to protect a child from the risk of ongoing abuse and the need to protect other children from serial offenders. There may be a great deal of pressure exerted on a clinician to say if a child is a virgin or not; indeed there may even be requests for certificates of virginity. Apart from the myriad of associated ethical issues there is no evidence base to determine with accuracy if a person has been sexually active or not. Many forms of abuse will not result in any injury and even when anogenital injuries are sustained they tend to heal quickly and completely. Knowledge of what services are available in the local area is important to ensure timely smooth referrals and ensure seamless care for this very vulnerable group. It is an abuse of power by those exploiting by virtue of their age, gender, intellect and physical strength and/or economic or other resources. As well as professionals being alert to the warning signs that a child is either a victim of exploitation or at risk of such, it is also crucial that the child or young person is not alienated by an interrogative style of history taking and any suggestion that they may to blame for what has happened to them by the decisions they have made. Section 11 of the Children Act 200411 places duties on a range of professionals including healthcare workers. It is clear that health professionals are in a strong position to identify welfare needs or safeguarding concerns regarding individual children and, where appropriate, provide support. This includes understanding risk factors, communicating effectively with children and families, liaising with other agencies, assessing needs and capacity, responding to those needs and contributing to multi-agency assessments and reviews. Clinicians should be familiar with the intercollegiate document, March 2014, Safeguarding children and young people: roles and competences for health care staff. The impact will depend upon many factors such as the nature of the abuse, who the abuser was, in terms of the abuse of power and trust, how long the abuse went on for, what other disadvantages a child was subject to , etc. Therefore victims will show a range of symptoms as a result of their abuse, with some seemingly having no long-term ill effects. Whilst much is often made of physical sequelae it is often the psychological effects that affect a victim the most. Some victims may suffer with low self-esteem, underperformance at school, self-harm or suicide. In addition to this some longer-term studies are revealing that child victims are at increased risk of physical illness including cardiovascular disease in adulthood. It states: this guidance aims to help professionals understand what they need to do, and what they can expect of one another, to safeguard children. It focuses on core legal requirements and it makes clear what individuals and organisations should do to keep children safe. Doctors must play a central role in this, acting as advocates for those without a voice, challenging myths and stereotypes, raising awareness of issues however unpalatable and seeking to eradicate the causes and perpetuation of the circumstances that allow such abuse to flourish. Working Together To Safeguard Children: A guide to interagency working to safeguard and promote the welfare of children. Prevalence and risk of violence against children with disabilities: a systematic review and meta-analysis of observational studies. Safeguarding children and young people: roles and competences for health care staff. Physical and sexual abuse in childhood as predictors of early-onset cardiovascular events in women. Section 1 covers the law and the basic competencies for the initial contact, management, examination, evidence collection and subsequent follow-up. In order to ensure exposure to the required case mix the unit must be of a sufficient size to ensure completion of the training. Frequently it remains a hidden problem and yet the sequalae may have profound effects on the physical and psychological health of the victim, both in the short and long term. It is important for clinicians to have an awareness of the scale of the problem, how it may present and then how to manage the situation. They should be able to respond to a direct disclosure of rape or sexual violence and also, perhaps more importantly, they should be alert to the possibility of sexual violence as the root cause of other presentations. Prevalence 823 Interpersonal violence may also cause ethical dilemmas for the clinician.
Levitra Professional Dosage and Price
Levitra Professional 20mg
- 10 pills - $60.63
- 20 pills - $80.81
- 30 pills - $101.00
- 60 pills - $161.55
- 90 pills - $222.11
- 120 pills - $282.66
- 180 pills - $403.77
These edges are called Geometric Edges erectile dysfunction doctors augusta ga purchase discount levitra professional on line, for example, b2 = (B1, B4) and b3 = (B1, B3). In addition, in order to avoid connecting similar attributes in a P-graph label, the Constrained Edge attempts to delete those edges with matching properties due to the repulsive interaction among different regions of the polypeptide chains [5]. These approaches operate when the same forces are opposition or the atoms are not closely bonded. Moreover, d is usually determined as the average of the distances between all pairs of atoms in the protein. In this manner, b1 is composed of the substructures of a helix and a sheet, and one of which is the polar component. The modular graph can be regarded as a technique of finding the maximum common subgraph of two given labeled graphs [31]. However, edges y and z will not exist in the modular graph as they do not satisfy the definition. Thus, the Jaccard similarity coefficient is adopted for our graph scoring function. The proposed method presents a convincing viewpoint, showing inferred evolutionary relationships among various strains. Attributes of edges are graded into three types, physical, geometric, and constrained edges. Adopting from several properties on vertices and edges, protein comparison could be improved by incorporating more specific parameters. It may be worth pointing out that the construction of P-graphs is limited by the number of secondary structures. However, in real applications, there is a small chance to locate an isomorphic relation between graphs. It has also been found that there is no efficient way for determining graph isomorphism. Hence, as already mentioned, graph spectra give an alternative solution to graph matching. The properties of topological relationships can be deduced from the graph spectra of the proteins being compared. One practical way to tackle this is to symbolize the graph as a matrix, turning it into numbers and vectors. In other words, 4, 4, 2, 0 (respectively, 4, 4, 1, 1, 0) is the eigenvalue multiset of X (respectively, Y). To measure the similarity of X and Y, these two vectors will be normalized into the same dimension, that is, X will become [4, 4, 2, 0, 0]. The distance between X and Y is defined as the Euclidean distance between X and Y, that is, 2 = 1. In Reference [43], the authors applied the minimum weight bipartite matching on the Laplacian spectra to determine the distance. For example, the bipartite matching distance between X = [4, 4, 2, 0] and Y = [4, 4, 1, 1, 0] is 1 as [4, 4, 2, 0] will match [4, 4, 1, 0] of [4, 4, 1, 1, 0]. In the following, we discuss the issue of which matrix is better for use in determining the similarity of two protein graphs. If M is a matrix obtained from a graph G, then the spectrum of M is also called the spectrum of G. If two graphs have the same spectrum, then they are cospectral (or isospectral) graphs. In this section, we compare four spectra of matrices to examine their accuracy in protein structural comparison. These four spectra are derived from the adjacency matrix, Laplacian matrix, signless Laplacian matrix, and Seidel adjacency matrix. An ordinary spectrum of a finite graph G is the spectrum of its adjacency matrix A. Apparently, comparing with the binary relation of G, the spectrum of G tends to enrich information on the adjacent relation. Let Cn (respectively, Kn and Sn) denote the cycle (respectively, complete and star) graph of n vertices. The spectra of X and Y (by their adjacency matrices) are identical, that is, X = Y = [2, 0, 0, 0, -2]. From the point of view of a topological relation, the spectra of adjacency matrices from X and Y should not be equal owing to their incompatible topologies. Therefore, the Laplacian matrix is proposed to improve the factors of the graph relation. It is the difference of the degree diagonal matrix and the adjacency matrix of the given graph. In this case, the spectra of X and Y are X = [4, 2, 2, 0, 0] and Y = [5, 1, 1, 1, 0], respectively. In this case, the spectra of X and Y are still X = [4, 2, 2, 0, 0] and Y = [5, 1, 1, 1, 0], respectively, that is, the spectra of the Laplacian and signless Laplacian matrices are equal for these two graphs. Although studies have found that the signless Laplacian matrix spectrum performs better than other commonly used graph spectra [14], most of the surveys were confined to combinatorial, graph-theoretical analysis, and linear algebra problems. It is modified from the adjacency matrix such that each entry si,i is 0, si,j is -1 if the vertices i and j are adjacent, and si, j is 1 if they are not adjacent [53] (see Eq.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.