
Lotrisone
General Information about Lotrisone
Another benefit of Lotrisone is that it is relatively safe to use. Side effects similar to itching, burning, or stinging on the site of utility are uncommon, and severe allergic reactions are very uncommon. However, as with any medication, you will want to follow the directions carefully and only use Lotrisone as directed by a physician or pharmacist.
Fungal infections can happen nearly anyplace on the body, from the scalp, feet, and nails, to the groin, hands, and even the inside of the mouth. They may be attributable to quite lots of fungi, together with dermatophytes, yeasts, and molds. These infections can often be tough to treat, and if left untreated, can result in critical issues. Thankfully, Lotrisone is here to assist.
The two energetic components in Lotrisone, betamethasone and clotrimazole, work in different methods to deal with fungal infections. Betamethasone is a sort of corticosteroid that helps to scale back irritation and alleviate symptoms corresponding to redness, swelling, and itching. Clotrimazole, however, is an antifungal agent that works by inhibiting the expansion of fungi, stopping them from reproducing and spreading. Together, these two ingredients work to supply fast-acting reduction and eliminate the supply of the an infection.
Lotrisone is a well-liked antifungal medication that has been extensively used for treating skin infections caused by numerous kinds of fungi. The energetic ingredients in Lotrisone, betamethasone and clotrimazole, work collectively to inhibit the expansion of fungi, offering aid from signs and helping to clear up the infection. This powerful mixture makes Lotrisone extremely effective in treating a wide range of fungal pores and skin infections, and it is strongly recommended by medical doctors and pharmacists alike.
In conclusion, Lotrisone is a safe, efficient, and handy treatment for fungal skin infections. Its mixture of betamethasone and clotrimazole makes it a robust weapon towards quite lots of fungi, providing quick relief from signs and promoting healing. However, it is necessary to notice that Lotrisone isn't really helpful for use in kids underneath the age of 17, or pregnant or lactating girls, unless particularly instructed by a physician. If you are experiencing symptoms of a fungal pores and skin an infection, consult your physician or pharmacist to see if Lotrisone is the best treatment for you.
In addition to its effectiveness in treating fungal skin infections, Lotrisone can be recognized for its ease of use. It may be utilized on to the affected area, and solely must be used once or twice a day, depending on the severity of the infection. Lotrisone additionally is out there in handy, transportable packaging, making it easy to take with you wherever you go.
One of the best issues about Lotrisone is that it is out there in numerous varieties, together with cream and lotion, making it suitable for a selection of pores and skin sorts and situations. Lotrisone cream is often used to treat infections that happen between the toes, while the lotion is extra suited for treating infections on bigger pores and skin surfaces. This versatility makes it a preferred selection amongst both sufferers and healthcare professionals.
Lotrisone has been confirmed to be extremely efficient in treating a variety of fungal skin infections, corresponding to athlete's foot, jock itch, ringworm, and yeast infections. It works by attacking the root cause of the an infection, offering fast relief from symptoms and stopping the infection from spreading. This not solely helps to alleviate discomfort but additionally hastens the healing process and reduces the chance of problems.
The sparganum has a longitudinal excretory canal and muscle bundles arranged in longitudinal and horizontal fascicles ("checkerboard" pattern) and lacks a scolex or internal organoid structures fungus gnats dunks purchase genuine lotrisone online. When it migrates, it leaves behind a tract of necrosis surrounded by chronic inflammation with abundant eosinophils. Cysticerci in the skin and subcutaneous tissue have a benign course but if they are localized in the eye may cause 178 blindness and if in the brain or heart may kill the patient. They have a cephalic and a caudal clear space and are 200 to 360 µm long and 5 to 9 µm wide. This is a feature that distinguishes them from Mansonella streptocerca, the other microfilaria that can be seen in the dermis. A pruritic papular rash (onchocercal dermatitis) with lichenification and pigmentary changes ("leopard skin") can result because of an inflammatory reaction to antigens from degenerating microfilariae. Obstruction of lymphatics by microfilaria can result in lymphadenitis or adenolymphocele (hanging groin). In later stages, the dense fibrous tissue contains only scanty chronic inflammatory infiltrate, foreign body giant cells, eosinophils, and focal calcifications. The most common species causing subcutaneous dirofilariasis in humans are Dirofilaria tenuis (endemic in south Florida), Dirofilaria ursi and Dirofilaria subserrate (North America), and Dirofilaria repens (Europe). The filaria has a thick multilaminated cuticle with external longitudinal cuticular ridges. If the parasite has been dead for a long time, degenerative changes might make identification difficult. The mature miracidia inside the ova have a ring-shaped nerve center and intensely basophilic gonadal cells. It consists of a papular pruritic rash that develops on areas covered by swimming suits, but cercarial dermatitis occurs on exposed areas. Cercarial dermatitis is caused by "nonhuman" species of schistosomes, which cannot complete their life cycle in humans and are destroyed shortly after skin penetration. Late cutaneous bilharziasis is rare and is caused by deposition of ova in the dermis in patients with severe systemic invasion by the major species of schistosome fluke (S. An overview: the changing face of cutaneous infections and infestations, Clin Dermatol 20:104108, 2002. Late cutaneous bilharziasis consists of papular or verrucous lesions that can develop in the genital and perigenital skin after the deposition of ova in the dermis. Cercaria may be identified in the epidermis only if the biopsy is taken soon after penetration. Late cutaneous bilharziasis is characterized by the presence of calcified or degenerating ova in the dermis associated with a surrounding palisading necrotizing granulomatous reaction with numerous eosinophils. The epidermis is hyperkeratotic, sometimes pseudoepitheliomatous, and may show draining sinuses (transepithelial elimination). Viral skin infections in the elderly: diagnosis and management, Drugs Aging 19:503514, 2002. Clinical manifestations and treatment considerations of herpes simplex virus infection, J Infect Dis 186:S71S77, 2002. Cutaneous tuberculosis: diagnosis and treatment, Am J Clin Dermatol 3:319328, 2002. Tropical dermatology: bacterial tropical diseases, J Am Acad Dermatol 54:559578, 2006. Fungal infections of the skin: infection process and antimycotic therapy, Curr Drug Targets 6:849862, 2005. The medically important dematiaceous fungi and their identification, Mycoses 34:118, 1991. The diagnosis of deep mycoses by morphologic methods, Hum Pathol 13:519533, 1982. AndrewCarlson Vasculitis is a histologic diagnosis defined as inflammatory cell infiltration and destruction of blood vessels. Clinically, cutaneous vasculitis can present in a panoply of morphologies that include urticaria, purpura, hemorrhagic vesicles, ulcers, nodules, livedo, infarcts, and digital gangrene. These findings may represent the cutaneous manifestation of systemic disease, or, as is the case in most instances, represent a benign self-limited, single-episode phenomenon. Specific clinical vasculitic entities do not always correlate exactly with mechanisms, and any patient with vasculitis may have a constellation of morphologic signs that overlaps with another clinical entity that prevents confident clinical diagnosis. Both of these classification criteria were not originally developed as diagnostic criteria for individual patients (particularly those with early disease) but for comparisons of groups of patients. A definitive diagnosis of vasculitis requires histologic confirmation in almost all cases because few vasculitic syndromes have pathognomonic clinical, radiographic, and/or laboratory findings. Nonetheless, a biopsy diagnosis of vasculitis cannot stand by itself, as it must be correlated with clinical history, physical and laboratory findings and/or angiographic features. Therefore, the classification of cutaneous vasculitis into specific syndromes is best approached morphologically by determining vessel size and principal inflammatory response. In the evaluation of cutaneous vasculitis, accurate histologic classification is the first step in arriving in reproducible diagnosis of specific vasculitic syndrome. In adults, the mean age of onset of vasculitis is 47 years, and among children, the mean age of onset is 7 years. Classification of cutaneous vasculitis can be initially based on vessel size(s) affected and extent of skin and subcutaneous involvement. The diagnostic yield of a skin biopsy is greatly influenced by the depth of the biopsy. In general, punch biopsy or excision biopsy extending into the subcutis is the preferred means to sample a vasculitic lesion in order to sample vessels of all sizes.
Colloids: Polygelatin solutions (Hemaccel fungi definition and pictures order lotrisone overnight, Gelofusion) are iso-osmotic with plasma. Maintenance of cardiac efficiency: When a large volume of fluid or blood is to be administered, the cardiac competence or efficiency should be ascertained otherwise there is a risk of overloading the circulation and cardiac failure. One or two large bore (14 or 16 gauge) cannula are inserted for volume replacement. Packed red blood cells (specific blood component), combined with normal saline, are used for hemorrhagic shock. Administration of oxygen to avoid metabolic acidosis: In the initial phase, administration of oxygen by nasal cannula at a rate of 6-8 liters per minute is enough but in the later phases, ventilation by endotracheal intubation may be necessary. Endotracheal intubation and mechanical ventilation may be needed for patients with septic shock. Pharmacological agents: Use of vasopressor drugs should be kept to a minimum, since peripheral vasoconstriction is already present. The role of vasoactive drugs, inotropes and corticosteroids in shock has been discussed in detail in connection with management of endotoxic shock. Control of hemorrhage: Specific surgical and medical treatment for control of hemorrhage should start along with the general management of shock. The specific management of each variety of obstetric hemorrhage has been outlined in the related chapters. Monitoring: Clinical parameters like skin temperature, visible peripheral veins can be helpful to assess the degree of tissue perfusion. Principles of management are: (a) to correct the hemodynamic unstability due to sepsis (endotoxin), (b) appropriate supportive care and (c) to remove the source of sepsis. This includes administration of antibiotics, intravenous fluids, adjustment of acid base balance, steroids, inotropes, prevention and treatment of intravascular coagulation and toxic myocarditis, administration of oxygen and elimination of the source of infection. Antibiotics: Endotoxic shock is most commonly due to Gram-negative organisms, so proper antibiotics should be administered in adequate doses. The choice of antibiotic will depend upon the sensitivity test but before the report is available, broad spectrum antibiotics covering Gram-positive, Gram-negative and anaerobic organisms should be started. Intravenous fluids and electrolytes: Septic shock associated with hemorrhagic hypotension should be treated by liberal infusion and blood transfusion. Alternatively, a rough calculation of the amount of fluid to be administered can be assessed by the volume of urinary output and its specific gravity. Oliguria with high specific gravity is an indication for liberal fluid administration, whereas a low specific gravity indicates fluid restriction. Bicarbonate should be administered to correct persistent metabolic acidosis (pH < 7. Further doses will depend on the clinical state of the patient and blood gas analysis result. Adrenaline, noradrenaline, dopamine and dobutamine have both inotropic and vasoconstrictive effects. Its main action is on -adrenoreceptors, increasing cardiac contractility and cardiac output without change in rate. In a dose of 1-3 µg Kg1 min1 it increases renal cortical plasma flow and glomerular filtration. Adrenaline is a very potent and agonist and is sometimes used in patients who do not respond to dopamine or dobutamine especially in septic shock. Diuretic therapy: To reduce fluid overload (preload) and pulmonary edema, diuretics should be used. Corticosteroids: Patients with severe sepsis develop systemic inflammatory response syndrome (see p. The dose recommended in septic shock is 50 mg of hydrocortisone per kg body weight. The advantages claimed are: (i) exerts an anti-inflammatory effect at the cellular level (ii) stabilizes lysosomal membrane (iii) counteracts anaerobic oxidative mechanism (iv) improves the regional blood flow (microcirculation) and thereby reverse the metabolic acidosis (v) exerts positive inotropic effect to improve cardiac efficiency and (vi) some vasopressor effect. Treatment of myocarditis: Myocarditis most often is associated with septic hypotension. Under exceptional circumstances when there is evidence of congestive cardiac failure or features of atrial fibrillation or flutter, digitalis may be administered. Elimination of source of infection: Surgical intervention should be done to eliminate the source of infection. Evacuation of the retained products of conception or hysterectomy for a case with septic abortion or puerperal sepsis should be done without delay. Hysterectomy has been advocated in unresponsive endotoxic shock following septic abortion or puerperal sepsis. Intensive insulin therapy is done in patients with severe sepsis and septic shock to maintain normal blood glucose level. These patients often develop hyperglycemia which further increases the risk of septicemia and death. Recombinant human-activated protein C therapy (Drotrecogin Alfa): Activated protein C is one endogenous protein that inhibits inflammation, thrombosis and promotes fibrinolysis. It reduces mortality in patients with severe sepsis as it reduces coagulopathy and inflammation. These functions can be adequately maintained provided the blood supply to the organs and the functional integrity of the nephrons (units of the kidney) remain adequate. The probable factors are: (1) Diminished number of septic abortion with liberalization of abortion laws (2) Judicious and early termination in severe preeclampsia (3) Better understanding of the pathophysiology and management of shock (4) Appropriate management of abruptio placenta (5) Facilities of blood transfusion. There is significant physiological and anatomical changes in the kidney during pregnancy (p.
Lotrisone Dosage and Price
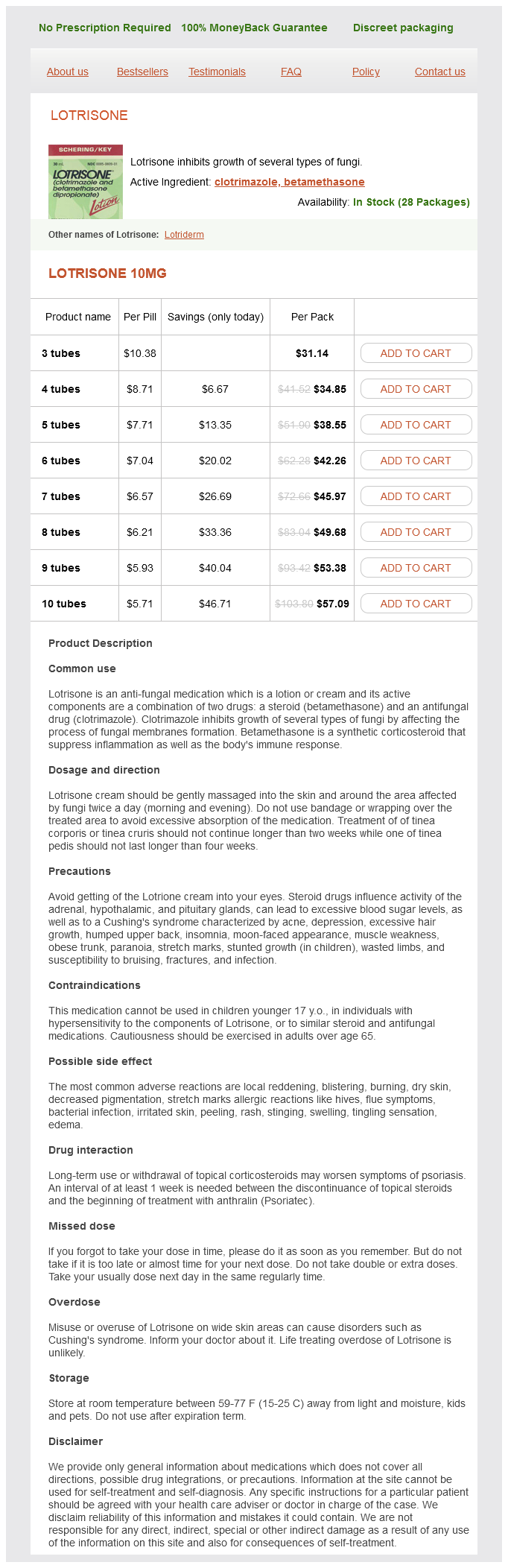
Lotrisone 10mg
- 3 tubes - $31.14
- 4 tubes - $34.85
- 5 tubes - $38.55
- 6 tubes - $42.26
- 7 tubes - $45.97
- 8 tubes - $49.68
- 9 tubes - $53.38
- 10 tubes - $57.09
Vaginal operative delivery in such cases may fungus kills ants lotrisone 10 mg order otc, at times, become risky producing trauma to the genital tract (complete perineal tear) or injury to the fetal head. There is compression of the occipitofrontal diameter with elongation of the vault at right angle to it. This type of molding favors tentorial tear because of extreme elevation of falx cerebri. There is also increased perinatal morbidity and mortality (10%) due to asphyxia or trauma during vaginal operative delivery. However, it is to be morbidity and remembered that in 4 out of 5 cases, there is usually no trouble and the fetus is delivered spontaneously. Apart from the overall assessment of the case, the pelvic assessment is mandatory. Inclination of the pelvis, configuration of the inlet, sacrum, ischial spines and the side walls are to be noted. Early cesarean section: Occipitoposterior per se is not an indication of cesarean section. Pelvic inadequacy or its unfavorable configuration, along with obstetric complications such as, preeclampsia, postcesarean pregnancy, big baby usually need cesarean section. First stage: In otherwise uncomplicated cases, the labor is allowed to proceed in a manner similar to normal labor. Forward leaning position (kneeling, hands and knees position) may help forward rotation and reduce back pain. Progress of labor is judged by-(a) progressive descent of the head (b) rotation of the back and the anterior shoulder toward the midline, (c) increasing exion of the head, (d) position of the sagittal suture on vaginal examination and (e) cervical dilatation. Weak pain, persistence of de exion and nonrotation of the occiput are the triad too often coexistent. Indication of cesarean section: (a) Arrest of labor (failure of rotation), (b) incoordinate uterine action and (c) fetal distress. Second stage: In majority, anterior rotation of the occiput is completed and the delivery is either spontaneous or can be accomplished by low forceps or ventouse. In minority (unrotated and malrotated): Provided the fetal and maternal conditions permit, one should take a watchful expectancy for the anterior rotation of the occiput and descent of the head. In such cases, proper conduction of delivery and liberal episiotomy should be done to prevent complete perineal tear. Third stage: Because of prolongation of labor, tendency of postpartum hemorrhage can be prevented by prophylactic intravenous ergometrine 0. Following vaginal operative delivery, meticulous inspection of the cervix and lower genital tract should be made to detect any injury. The case is once more to be assessed abdominally and vaginally before formulating the suitable method of interference. The cup is placed more toward the occiput to promote flexion and the rotation is expected during its descent on traction (see p. The pelvis should be adequate; the baby is of average size and there is good amount of liquor. Its advantages over manual rotation are-(1) no chance of displacement of the head, (2) accidental cord prolapse is absent and (3) rotation can be done at, above or below the level of obstruction-depending upon the type of pelvis. If the occiput remains at or above the level of ischial spines, cesarean section should be considered. The arrest in occipitotransverse position may be the end result of incomplete anterior rotation (1/8th of circle) of oblique occipitoposterior position, or it may be due to nonrotation of the commonly primary occipitotransverse position of normal mechanism of labor. Causes: (a) Faulty pelvic architecture such as prominent ischial spines, flat sacrum and convergent side walls, (b) Deflexion of the head, (c) Weak uterine contraction, (d) Laxity of the pelvic floor muscles. Diagnosis: (a) the head is engaged, (b) the sagittal suture lies in the transverse bispinous diameter, (c) Anterior fontanel is palpable, (d) Faulty pelvic architecture may be detected. Management: the fetal condition and pelvic assessment give the guide as to the line of management (mentioned earlier). If a big caput has been formed, the direction of the unfolded pinna of the ear which points toward the occiput, can be taken for help. The corresponding hand is introduced into the vagina in a cone-shaped manner after separating the labia by two fingers of the other hand. In occipitotransverse position, the four fingers are pushed in the sacral hollow to be placed over the posterior parietal bone and the thumb is placed over the anterior parietal bone. By a movement of pronation of the hand, the head is rotated to bring the occiput anterior along the shortest route. A little over rotation is desirable anticipating slight recurrence of malposition before the application of forceps. When the left hand is used, it is placed on the right side of the pelvis after rotation, as such the right blade is to be introduced first and the left blade is then to be introduced underneath the right blade. Difficulties and dangers: the difficulties are due to-(1) Failure to grip the head adequately due to lack of space, (2) Failure to dislodge the head from the impacted position, (3) Inadequate anesthesia, (4) Wrong case selection. In this method, the four fingers and not the thumb are introduced into the vagina. Its advantages over the whole hand method are: (i) less space is required and (ii) less chance to displacement of the head. The four fingers are introduced into the vagina and tangential pressure is applied on the head at the level of diameter of engagement. The force is applied intermittently till the occiput is placed behind the symphysis pubis. Simulated learning using mannequins and model pelvis with an experienced trainer is needed to acquire the skill. In favorable circumstances (90%) occiput rotates anteriorly 3/8th of a circle anteriorly and delivery occurs as in occiput anterior.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.