
Mentat
General Information about Mentat
One of the primary advantages of Mentat is its capability to enhance memory and studying talents. The components in Mentat work collectively to boost the production of acetylcholine, a neurotransmitter that's important for learning and reminiscence. This results in better retention of data, increased focus, and improved general cognitive skills. Additionally, Mentat contains essential fatty acids that support the growth and upkeep of mind cells, preserving the mind in good situation and protecting it from age-related decline.
Mentat is a unique psychological health formula that has gained popularity in current times. It is a natural supplement that supports brain operate in each normal and demanding situations. The word “Mentat” originated from the fictional world of Frank Herbert’s “Dune” novels, the place it was used to explain a gaggle of people with enhanced cognitive talents. Although Mentat may not offer you superhuman cognitive powers, it's definitely a powerful complement that may help you keep a healthy and sharp thoughts.
Another noteworthy function of Mentat is its neuroprotective properties. The energetic components in Mentat have been discovered to have antioxidant and anti-inflammatory properties, lowering oxidative stress and irritation in the brain. This might help to stop age-related cognitive decline and even protect the mind from neurodegenerative illnesses like Alzheimer's and Parkinson's.
Mentat is a protected and natural complement that does not require a prescription. However, it's all the time advisable to seek the guidance of a healthcare skilled earlier than incorporating any new supplement into your routine, particularly if you're on any treatment or have an underlying medical condition. Additionally, the really helpful dosage must be adopted to keep away from any potential unwanted side effects.
In conclusion, Mentat is an excellent mental fitness method that can profit individuals of all ages and lifestyles. Its pure and high-quality ingredients make it a protected and preferable option for those seeking to enhance their cognitive talents. With regular use, Mentat can help you to take care of a wholesome and sharp thoughts, even in the face of demanding and tense conditions. So, if you need to keep mentally fit and sharp, give Mentat a attempt to experience the advantages for yourself.
Mentat isn't just for those looking for to improve their cognitive operate. It can be useful for people who have a demanding lifestyle that requires them to be alert and targeted for extended intervals. Busy professionals, college students, and even athletes can benefit from Mentat's capability to boost mental efficiency beneath annoying conditions. The complement not solely helps to alleviate stress and nervousness but in addition boosts mental endurance, permitting individuals to stay sharp and targeted for longer durations.
In right now's fast-paced world, our brains are constantly bombarded with info, duties, and stress. This can take a toll on our mental well being and cognitive perform. As we age, we might experience reminiscence loss, issue focusing, and psychological fatigue. While there are many brain-enhancing supplements obtainable out there, Mentat stands out as a pure and safe choice.
Mentat is a product of the famend company, Himalaya Herbal Healthcare. The firm has been in the herbal complement business for over 90 years and has a popularity for utilizing high-quality and pure elements. Mentat is made from a blend of herbs and minerals which have been utilized in traditional Ayurvedic medication for centuries. This blend includes Bacopa Monnieri, Centella Asiatica, Convolvulus Pluricaulis, and different natural components which were scientifically confirmed to enhance mind perform and reminiscence.
The decision to wait for consultants is best made by the emergency physician at the bedside and should be based on clinical judgment symptoms 8 days before period purchase mentat line. In 2012, Halpern and colleagues introduced a scoring system based on effusion size, echocardiography derangements, and clinical criteria. The clinician who performs the procedure should be the one who is most experienced in both sonography and pericardial fluid aspiration. Tamponade Caused by Nonhemorrhagic Effusions Most nonhemorrhagic effusions are liquid. They can be drained by pericardiocentesis with a small needle or by a catheter left in the pericardial space. Removal of even a small amount of fluid can cause immediate and dramatic improvement in blood pressure and cardiac output. Pericardiocentesis relieves tamponade caused by nonhemorrhagic effusions in 60% to 90% of cases. Placement of a pericardial catheter is more useful in the longterm management of these patients. Therefore if time and patient stability permit, consider pericardiocentesis with a catheter to reduce the necessity for repeated aspirations. Without signs of tamponade, however, these patients may be better managed by dialysis. In one series, 63% of renal failure patients were managed successfully with only dialysis. Pericardiocentesis in Patients With Hemorrhagic Tamponade For hemorrhagic tamponade, pericardiocentesis is never the definitive treatment because this strategy has several drawbacks. A study investigating traumatic cardiac injury found that all patients who underwent surgery within 2 hours of the injury survived but the mortality rate was higher in patients who experienced longer operating room delays. The number of deaths from stab wounds has been decreasing over time in response to a shift in trauma philosophy in which early thoracotomy is supported rather than repeated pericardiocentesis. A study of penetrating trauma patients with tamponade found that preoperative pericardiocentesis decreased the mortality rate from 25% to 11%. No Consider other diagnosis Fluid challenge Sympathomimetics Pneumatic trousers Consider subxiphoid pericardiotomy Yes Admit Urgent dialysis No Known renal failure Although the procedure can be done with these two simple devices, access to several others would be beneficial during the procedure. Of all the components, the most essential is an ultrasound machine, which first is used to determine whether a pericardial effusion is present and then assists in accurate needle placement. Before the introduction of real-time sonography to guide needle placement, electrocardiographic monitoring was used to indicate appropriate needle placement. This is done by connecting the electrocardiographic machine to one of the precordial leads. Ideally, pericardiocentesis is performed in the cardiac catheterization laboratory under fluoroscopic or echocardiographic guidance. With the advent of bedside ultrasound and immediate visualization of large pericardial effusions, pericardiocentesis is being performed in the Ed more frequently. Most patients undergoing pericardiocentesis in the Ed have already experienced hemodynamic collapse and are lying supine. If the patient is able to cooperate, elevate the chest 30 to 45 degrees to bring the heart closer to the chest wall. Sedation of stuporous patients is typically forgone because of the risk for further hemodynamic collapse. If the patient is awake and undergoing the procedure without obvious hemodynamic compromise, short-acting medications. Prepare the chest and upper part of the abdomen with a chlorhexidine-based solution. If the patient is awake, anesthetize the skin and the proposed route with 1% lidocaine (see Review Box 16. Pericardial fluid is not always distributed circumferentially in the pericardial sac, so ultrasound can quickly identify the maximal effusion pocket and demarcate the appropriate site for needle placement. Pericardiocentesis with ultrasound guidance is currently the safest and most reliable method for the diagnosis and treatment of pericardial effusion and tamponade. However, these studies also revealed that an apical approach is associated with a greater incidence of pneumothorax than a traditional subcostal approach is. Before the advent of ultrasound guidance, the subxiphoid approach (discussed later in this chapter) was the preferred method of pericardiocentesis. It is still used frequently during cardiac arrest and when ultrasound is not readily available. The precordial lead can then be used as a rhythm strip to monitor the needle tip continuously. Other tools that are desirable for urgent pericardiocentesis can be found easily in the Ed or in a pericardiocentesis kit (see Review Box 16. Therapy typically consists of either pericardial drainage by needle aspiration or placement of a pericardial window. These procedures are not classically performed in an Ed, so temporizing methods are the mainstay of therapy unless the patient is unstable. The most common therapeutic procedures used as temporizing measures in the setting of tamponade are intravascular volume expansion with crystalloids and administration of vasopressors or inotropes. Fluid resuscitation in a trauma patient with penetrating cardiac injury might cause deterioration. Animal experiments indicate that the response depends on whether fluid boluses produce recurrent bleeding from the cardiac wound. Norepinephrine, isoproterenol, dopamine, and dobutamine have all been evaluated as the vasopressor or inotropes of choice in patients with cardiac tamponade. Norepinephrine and isoproterenol increased cardiac output in animal models of tamponade, but failed to increase it in humans.
During later infections medicine - mentat 60 caps otc, as the parasite fed on a root vegetable diet (such as in France, where invades muscle tissue, elevated white blood cells are trichinosis is rare). Increased levels of creatine kinase and lactate dehydrogenase (which indicate muscle cell Symptoms damage) are seen in blood tests, but these are not speSymptoms of trichinosis vary depending on the part of cific to trichinosis. If the infection Specific tests are available that measure antibodies to is in the intestine, symptoms include nausea, diarrhea, the parasite. These are indirect immunofluorescence, vomiting, fatigue, fever, and stomach pain. Symptoms latex agglutination, and enzyme-linked immunosorexperienced as the parasite reaches other parts of the bent assays; but these are not useful until a minimum of body include headaches, chills, cough, painful joints, three weeks after infection and may give false-positive muscle aches and inflammation, and swelling of the results in persons with other infections or with autoimeyes. Screening and Diagnosis Adult worms in the gastrointestinal tract can be elimiThere is no test to diagnose the early (intestinal) nated with the use of thiabendazole, mebendazole, or stages of Trichinella infection. These are effective within one week of 1072 · Trichomonas infection and are used to prevent further infection by the parasite. Once the parasite has invaded tissues, inflammation at infection sites is treated with prednisone. Prevention and Outcomes Trichinosis is prevented by thoroughly cooking pork and pork products. Recommended temperatures for freezing are 5° for twenty days, minus 10° for ten days, or minus 20° for six days (for a six-inch piece of meat). This article summarizes the basic science of Trichinella infection and provides clinical information on trichinosis. This article examines trichinosis and discusses the economic importance of eliminating the parasite from the food chain. The tissue nematodes section of this chapter includes discussion of trichinosis, which also includes its etiology, pathogenesis, and epidemiology. In addition to an overview of the disease, this article discusses the Trichinella species, including its life cycle. It is a symptomatic infection of the vaginal tract in women and a usually asymptomatic infection of the urethra in men. Causes Trichomonas is caused by infection with the singlecelled protozoan parasite Trichomonas vaginalis, which is transmitted almost exclusively through vaginal sexual intercourse. Extremely rare cases of fomite transmission, that is, transmission through a contaminated object, have been reported. Risk Factors Risk factors for contacting trichomonas include those things that increase the chances of contact with an infected partner. Persons with multiple sexual partners, who have unprotected sexual intercourse, and who have untreated sexual partners are at high risk. In addition to the noted risk factors for trichomonas, associated high risks have received focused attention from researchers. Symptoms In women, trichomonas symptoms include a foamy grayish discharge with a foul odor; mild, moderate, or intense itching and burning that often includes pain with intercourse; and, in severe cases, erythema (redness) of the vagina and inner vulvar folds. Some women may experience pain with urination and may confuse their symptoms with that of a urinary tract infection. Men are usually asymptomatic, but men who do have symptoms present with penile burning on urination, a reddened urethral opening, and a clear penile discharge that is often misdiagnosed as nongonococcal urethritis or chlamydia. This misdiagnosis can result in the provision of antibiotics that are effective against chlamydia but that have no treatment value for trichomonas. Symptoms may present anywhere from a few days to a month following transmission, so for persons with multiple partners, there is often no way to determine when the infection was acquired based on symptoms. Infection in women is marked by an increased pH (acidity) of the vaginal fluid in most cases, so screening women who are undergoing vaginal speculum examinations with pH paper has been suggested. For many years the gold standard for diagnosis has been the saline wet prep, which requires a working microscope, skill in examining wet prep specimens, and a laboratory certification for the clinical setting Trichomonas · 1073 for provider-performed microscopy. Specificity refers to a lack of false-positive results and is especially important for a sexually transmitted infection that can raise serious issues in a relationship. Sensitivity is increased by scanning multiple fields and by examination immediately after collection of a specimen, because the organisms may die quickly. Because of these limitations, many clinical settings have not always been able to offer wet prep testing, and laboratory diagnostic testing methodologies have become available with send-out and point-of-care testing. Pap screening may also produce incidental findings of trichomonal organisms, but because of a high rate of false-positive results (low specificity), this should only be treated as a screening, rather than a diagnostic finding, so confirmatory testing is required. Culture is also available in a few specialty laboratory settings, utilizing vaginal secretions in women and urine, urethral swabs, or semen in men. In laboratories that have the capability of centrifuging urine and doing a microscopic examination of the spun sediment, trichomonal organisms, or trichomonads may be identified in male urine sediment. Diagnosis is usually made from testing symptomatic women through a wet prep of vaginal discharge. Treatment and Therapy Trichomonas is a curable sexually transmitted infection, without a high rate of relapse if partners are properly treated and if future behavioral changes can be implemented. Treatment is generally with only two approved medications: metronidazole in a single 2 gram (g) oral dose, or tinidazole in a single 2 g oral dose. Alternatively, metronidazole can be given as one 500 milligram tablet twice each day for seven days. Persons who are treated with a one-dose regimen are given multiple tablets (often four).
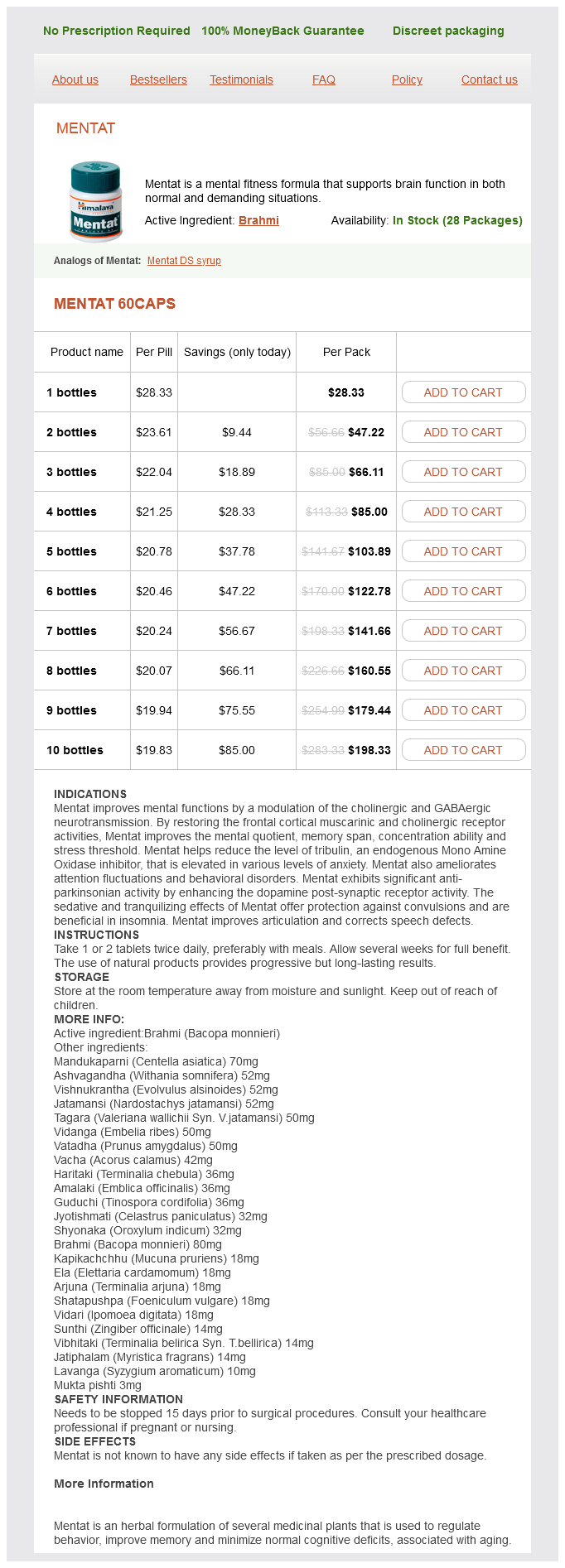
Mentat Dosage and Price
Mentat 60caps
- 1 bottles - $28.33
- 2 bottles - $47.22
- 3 bottles - $66.11
- 4 bottles - $85.00
- 5 bottles - $103.89
- 6 bottles - $122.78
- 7 bottles - $141.66
- 8 bottles - $160.55
- 9 bottles - $179.44
- 10 bottles - $198.33
Because these patients tend to progress to high-degree block without warning symptoms vaginitis order mentat 60 caps line, a pacemaker is often placed prophylactically. Some patients are prophylactically Sinus Node Dysfunction Bradycardias paced on a temporary basis, even in the absence of hemodynamic compromise. These conduction abnormalities frequently result in hemodynamically tolerable escape rhythms because of sparing of the bundle branches. A hemodynamically unstable patient who is unresponsive to medical therapy should be paced promptly. Whether and when stable patients should be paced is unclear, but placing a transcutaneous pacer is one option that can be attempted before placing a transvenous pacing catheter. Pacing is not a standard intervention in traumatic cardiac arrest, but in selected cases it may be considered. Several rhythm and conduction disturbances have been documented in patients with nonpenetrating chest trauma. In these patients, traumatic injury to the specialized conduction system may predispose to life-threatening dysrhythmias and blocks that can be treated by cardiac pacing. Transvenous pacing is also useful in patients with digitalis-induced dysrhythmias, in whom direct current cardioversion may be dangerous, or in patients in whom there is further concern about myocardial depression with drugs. Because these drugs have direct effects on cells of the myocardial pacemaker and conduction system, cardiac pacing is usually of little therapeutic value. Tachycardic rhythms from amphetamines, cocaine, anticholinergics, cyclic antidepressants, theophylline, and other drugs do not benefit from cardiac pacing. Drug-induced torsades de pointes may theoretically be overdriven by pacing, but data on this technique are lacking. Cardiac pacing is not used for bradycardias from these sources; rather, the underlying central nervous system depression is addressed. Severe bradycardia and heart block often accompany overdose of digitalis preparations, -adrenergic blockers, and calcium channel blockers. Although intuitively attractive, cardiac pacing is not generally effective for serious toxin-induced bradycardias, even though there have been rare case reports of success. Worsening of blood pressure may occur as a result of loss of atrial contractions with ventricular pacing. Likewise, calcium channel blocker overdose and digitalis-induced bradycardia and heart block rarely benefit from cardiac pacing. Pharmacologic interventions, such as digoxin-specific Fab, glucagon, calcium, inotropic medications, and vasopressors, remain the mainstay in the treatment of drug-induced dysrhythmias. Given the lack of success of pacing, possible downsides, and the greater effectiveness of specific antidotes, it is not standard to routinely attempt transvenous cardiac pacing in the setting of drug overdose. Indications of temporary and permanent pacemaker insertion, Circulation 58:690, 1978. Since 1980 there has been increasing interest in pacing therapy for symptomatic tachycardias. Supraventricular dysrhythmias, with the exception of atrial fibrillation, respond well to atrial pacing. By "overdrive" pacing the atria at rates 10 to 20 beats/min faster than the underlying rhythm, the atria become entrained, and when the rate is slowed the rhythm frequently returns to normal sinus. Because ventricular fibrillation under these conditions is difficult to convert, caution is advised when considering pacing severely hypothermic and bradycardic patients. Equipment Several items are required to insert a transvenous pacemaker adequately. The usual components required to insert a transvenous cardiac pacemaker are depicted in Review Box 15. Pacing Generator Many different pacing generators are available, but in general they all have the same basic features. The controls will frequently have a locking feature or cover to prevent the generator from being switched off or reprogrammed inadvertently. An amperage control allows the operator to vary the amount of electrical current delivered to the myocardium, usually 0. Increasing the setting increases the output and improves the likelihood of capture. The pacing control mode is determined by adjusting the gain setting for the sensing function of the generator. By increasing the sensitivity, one can convert the unit from a fixed-rate (asynchronous mode) to a demand (synchronous mode) pacemaker. The typical pacing generator has a sensitivity setting that ranges from approximately 0. The voltage setting represents the minimum strength of the electrical signal that the pacer is able to detect. Decreasing the setting increases the sensitivity and improves the likelihood of sensing myocardial depolarization. In the fixed-rate mode, the unit fires despite the underlying intrinsic rhythm; that is, the unit does not sense any intrinsic electrical activity. Temporary pacing generators are battery operated, and thus it is always good practice to install a fresh battery whenever pacing is anticipated. Pacing Catheters and Electrodes Several sizes and brands of pacing catheters are available.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.