
Mildronate
General Information about Mildronate
The controversy surrounding mildronate stems from its inclusion on the World Anti-Doping Agency's (WADA) listing of prohibited substances. It was added to the record in 2016 after several high-profile athletes, together with tennis star Maria Sharapova, examined optimistic for the drug. WADA claimed that mildronate was getting used as a performance-enhancing drug, regardless of there being no proof to assist this declare.
Aside from its use in treating heart ischemia, mildronate has additionally been accredited for use in neurology for the remedy of mind circulation problems. These situations, such as strokes or transient ischemic assaults (TIA), occur when there is a momentary interruption in blood circulate to the brain. This can outcome in signs corresponding to numbness, weak spot, or problem talking.
Additionally, mildronate has been found to have positive effects on learning skills and reminiscence. In a study performed on rats, those treated with mildronate showed higher efficiency in learning and memory tasks compared to the management group. This is because of the drug's ability to extend oxygen provide to the brain, which is important for optimal brain operate.
It is essential to notice that the use of mildronate must be beneath the supervision of a medical skilled. Like any treatment, it may cause unwanted effects such as headache, nausea, and belly ache. It is also not recommended for use in pregnant or breastfeeding people.
In conclusion, mildronate is a medication that has been used for decades to deal with heart ischemia and brain circulation problems. It has proven to have optimistic results on patients' mood, motor function, and cognitive skills. While its inclusion on the list of banned substances has brought on controversy, the drug's advantages for those suffering from these circumstances shouldn't be missed. As always, it is necessary to seek the guidance of a medical skilled earlier than taking any medicine.
Mildronate, also recognized as meldonium, has become a topic of interest in latest times due to its use by professional athletes and the controversy surrounding its performance-enhancing results. However, this drug has been around for the rationale that Seventies and was originally developed as an anti-ischemic medication for the remedy of coronary heart ischemia and its consequences.
Mildronate works by inhibiting a substance called gamma-butyrobetaine hydroxylase, which performs a job in the manufacturing of carnitine. Carnitine is a compound that helps the body convert fat into vitality. By inhibiting the production of this enzyme, mildronate will increase the degrees of available carnitine within the physique, permitting for improved power manufacturing and elevated oxygen supply to the heart muscle.
Heart ischemia is a condition the place there is a lowered blood provide to the guts muscle. It occurs when the coronary arteries, which provide oxygen-rich blood to the guts, turn out to be slim or blocked. This can result in symptoms similar to chest ache, shortness of breath, and fatigue. If left untreated, coronary heart ischemia can lead to extra serious circumstances corresponding to a coronary heart attack or coronary heart failure.
Studies have shown that mildronate can significantly improve the temper of patients with mind circulation issues. They turn out to be extra lively, their motor dysfunction decreases, and signs similar to asthenia (weakness), dizziness, and nausea turn into less pronounced. This can tremendously improve the quality of life for these sufferers and help them regain their independence.
Otherwise medicine side effects purchase mildronate 250 mg with mastercard, a combination of haloperidol and promethazine is recommended;3 it allows lower doses of both agents to be used, but risks adverse effects from both agents. If medicines are being used off-license, the prescriber should take full responsibility, informed consent should be obtained and documented, and relevant professional guidance should be followed. Maximum of three injections/day and 30 mg/day (including all formulations) 5 mg (range 210 mg), repeated after 4 hours. Maximum of 18 mg/day 50 mg (may be repeated once after 12 hours) 378 Rapid tranquillisation considering moving from oral to intramuscular (only if two doses fail or the person or others are at significant risk), or intramuscular to intravenous administration. In this scenario, specific rationale and risk assessment should be documented; consultation with expert peers may be useful. An advance directive is in place indicating this is a preferred management strategy. Risks Risks include extrapyramidal adverse effects (especially acute dystonia), oversedation (leading to loss of consciousness/alertness), loss of airway, cardiovascular/respiratory collapse, seizures, neuroleptic malignant syndrome, sudden death, interaction with other medication/substances, issues with comorbidities, injury to the service user/staff and a negative effect on the therapeutic relationship. Any issues detected should prompt increased monitoring, withholding of additional medication and early medical referral. Serum creatinine alone is not an accurate measure of renal function, as it is affected by factors independent of renal function, including age, gender, race and body size. For this reason, prediction equations using serum creatinine are commonly used to estimate renal function in practice. Creatinine clearance the most commonly used method for determining CrCl is the Cockcroft and Gault equation:1 F × (140 age) × weight (kg) CrCl (mL/ min) = serum creatinine (micromol/L) where F = 1. Renal function gradually declines with age; however, this may not result in an elevated serum creatinine due to a concurrent reduction in muscle mass. Both have the same serum creatinine, but the 70-year-old female has a CrCl of 22 mL/min, whereas the 30-year-old male has a CrCl of 68 mL/min. Most recommendations for dose adjustment in patients with renal impairment are based on CrCl calculated using Cockcroft and Gault. The risks of drug toxicity or therapeutic failure in an individual patient must always be considered and neither method is validated in acutely unwell patients. R Measuring CrCl from a serum creatinine concentration and a timed urine collection may be used to estimate renal function in situations where prediction equations may be inaccurate. A single serum creatinine measurement is taken and urine collected over a fixed period of time, usually 24 hours. The accuracy of a timed urine collection depends on the accurate collection of urine over the time period, which many patients find difficult and inconvenient. Using standardized serum creatinine values in the Modification of Diet in Renal Disease Study equation for estimating glomerular filtration rate. Renal disease: dosing in renal impairment and renal replacement therapy the kidney is an important site of excretion for many drugs and/or their metabolites. Reduction in renal function can significantly increase serum concentrations of renally excreted drugs and/or metabolites and cause accumulation and toxicity. A number of other pharmacokinetic and pharmacodynamic changes also occur in renal impairment that may alter efficacy and increase the likelihood of adverse effects. Phosphate binders/ion exchange resins may chelate drugs and reduce absorption. Only significant for water-soluble drugs with volume of distribution (V d) <1 L/kg. Clinically important for highly protein-bound drugs (>80%) such as phenytoin and warfarin. Care when interpreting drug levels for highly protein-bound drugs need to consider increased free levels. Renal impairment and renal replacement therapy 383 Metabolism Hepatic metabolic pathways are generally unaffected, although impact of renal impairment on accumulation of renally cleared active/toxic metabolites needs to be considered. Reduced doses of exogenous insulin are required in diabetics as renal function declines. Many water-soluble drugs and/or metabolites are excreted by the kidney and renal impairment may lead to reduced excretion, accumulation and toxicity unless dose and/or frequency are adjusted. Drugs that are most affected are those with significant renal excretion or active/toxic renally excreted metabolites. Table R2 illustrates how to manage some issues of excretion of drugs; dose reduction depends on: degree of renal impairment proportion of the drug and/or metabolites cleared by renal excretion toxicity therapeutic index. R Pharmacodynamic changes Uraemia and renal impairment can increase the risk of side effects of some medications, including: increased cerebral sensitivity to sedating medications (even if excretion unaffected) due to increased permeability of bloodbrain barrier. For drugs requiring rapid therapeutic levels that have a prolonged half-life in renal failure. What Factors Need to be Considered When Dosing Patients on Renal Replacement Therapies Proteinuria: leakage of protein into urine may occur when the glomeruli of the kidney are damaged. Cardiovascular disease: hypertension and chronic fluid overload can lead to left ventricular hypertrophy and cardiac dysfunction. Uraemia: accumulation of waste products such as urea can cause nausea, fatigue, itching, restless-leg syndrome and anorexia. Anaemia due to: Reduced erythropoietin production Iron deficiency (poor intake, poor absorption, increased losses) Renal bone disease: vitamin D from diet and sunlight (colecalciferol) requires hydroxylation by the liver and kidneys to become active (1,25-dihydroxycolecalciferol, calcitriol). Acidosis: the kidney regulates acid balance through reabsorption of bicarbonate and production of other buffers to remove hydrogen ions. Metabolic acidosis can occur when the kidney is unable to perform these functions. Dietary intervention: restrict/limit potassium, phosphate, salt and fluid intake where appropriate. Offer antiplatelet medication where appropriate, but be aware of increased risk of bleeding Itching: control phosphate and calcium levels; hydrate skin with topical moisturisers; sedating antihistamines Restless-leg syndrome: correct iron deficiency; clonazepam; haloperidol; ropinirole Nausea: antiemetics such as metoclopramide or prochlorperazine Gout: allopurinol Low-potassium diet Review medications, i.
Ulcerative colitis involves only the colon medications hyperkalemia discount 500 mg mildronate amex, beginning in the rectum and extending proximally in a confluent fashion. Ulcerative colitis is a mucosal disease, affecting deeper layers only if there is ulceration of mucosa over a broad front, accompanied by fulminant colitis. Currently there is no irrefutable proof of a single causative organism for either disease and it is more likely that they are caused by aberrant immune responsiveness to bacterial stimulation in the intestines. Her surgeon warns her that she runs the risk of developing severe problems due to malabsorption, such as osteomalacia and other vitamin deficiencies if the disease continues to involve her duodenum and small bowel. The surgeon warns her that her son may require investigation since inflammatory bowel disease can be familial. She has noticed that over the past few months her face has become rounder and that her cheeks have become redder. In particular, she is perturbed by the development of a small quantity of facial hair. She has put on weight around her abdomen but is puzzled by this because her upper arms seem to be thinner despite the fact that she takes regular exercise (although she has found this harder to do since the problems began). Overall, she does not feel in good health and is concerned that something serious is wrong. Examination confirms the physical features that the patient has already described, as well as revealing a fat pad on the upper aspect of the back and neck. The enlarged pituitary protrudes from the surface normally it is hidden inside the invaginated sella turcica. This technique relies on the fact that lipid-containing lesions drop in signal on the out-of-phase sequence. This is due to the natural, but weak, mineralocorticoid properties of glucocorticoids. Hence, there can be hyperkalaemia and hyponatraemia, both usually of a mild degree. In general, glucocorticoids function to elevate blood glucose and to mobilize fat and amino acids, especially from the periphery. This mobilization of proteins and lipids from the periphery (to an extent towards the central organs and tissues) can explain many of the clinical features, including easy bruising due to skin fragility and muscle weakness secondary to muscle protein loss. Answer 5 this question can be answered by considering the normal regulation of corticosteroid production. All of this means that interpreting a single cortisol level is problematic because it is difficult to establish what the normal range should be. Nevertheless, there are situations in which a single cortisol level can be of use in guiding things in the right direction (for example, a very low level would be unusual except in exogenous corticosteroid administration). Many of the causes are due to underlying mass lesions, so imaging can be of use in finding a mass lesion, but pituitary microadenomas are more difficult to discern. This may either be a microadenoma (under 10 mm) or a macroadenoma derived from the normal glandular cells of the anterior pituitary gland. Answer 10 Small cell carcinoma of the lung is derived from bronchial neuroendocrine cells. Many of the clinical features can be predicted from knowledge of the normal physiological functions of the involved hormones. The causes primarily centre around neoplasia and illustrate that a neoplasm, either benign or malignant, can retain some of the secretory functions of the tissue of origin. Furthermore, a neoplasm may acquire secretory functions that are not those of the underlying organ and yield a paraneoplastic syndrome. Unfortunately, her fatigued, hung-over and shattered state would count as no excuse with the professor of respiratory medicine, Roland Paul, and the prospect of having to repeat the six-week attachment was even more onerous to Sarah than the idea of having to leave the comfort of her bed that day. She did not even dare to entreat a little sympathy from the professor as he would be likely to regale her, plus any patient who was unfortunate enough to be captive in the consultation room, with a 45-minute anecdote regarding his antics as a medical student and how he had once Miliary tuberculosis Brain Lung Kidney Primary tuberculosis Lung: ghon focus plus hilar lymph node enlargement (primary complex) Terminal ileum: due to ingestion of milk infected by bovine tuberculosis A Sarah McKenzie Case passed his fourth-year exams with flying colours despite having imbibed enough whiskey to render an elephant unconscious. Feeling like her inner ears were now so sensitive she could detect anybody stamping their foot within five miles, Sarah tentatively sat down in a chair outside the clinic to await the arrival of the professor. Professor Paul arrived punctually and beckoned Sarah into the consulting room with him. The first patient was a 29-year-old woman who had recently been diagnosed as having tuberculous lymphadenitis of a right neck lymph node and was attending to receive the diagnosis and to have her treatment explained to her. Answer 1a Tuberculosis is an infection with the organism Mycobacterium tuberculosis. Mycobacteria, however, can live in the phagosome and prevent the fusion of lysosomes with the phagosome and so they are protected from the toxic contents of the lysosome. This capacity of mycobacteria to survive phagocytosis renders neutrophils ineffective against them and requires macrophages to resort to other strategies. Answer 1b When faced with an organism or inanimate substance that resists normal phagocytosis, macrophages can become further activated to form giant cells. This process requires co-ordination by T lymphocytes and results in multiple macrophages fusing together to form a single giant cell that has multiple nuclei and the ability to handle more stubborn phagocytic targets. The presence of granulomas and fibrosis within an organ results in the replacement of normal tissue, particularly if there is the accompanying destructive element of caseous necrosis. In addition, the cytokine production that is part of the granulomatous response may also have effects on adjacent tissue. This can occur with sufficiently little organ damage so that it is asymptomatic, or presents only as a cold-like illness. The precise factors that determine why reactivation happens are uncertain in many people, although a degree of immune suppression, such as the use of corticosteroids, is relevant in some. The granulomatous and fibrotic process once again occurs, but this time does not so readily contain the organisms.
Mildronate Dosage and Price
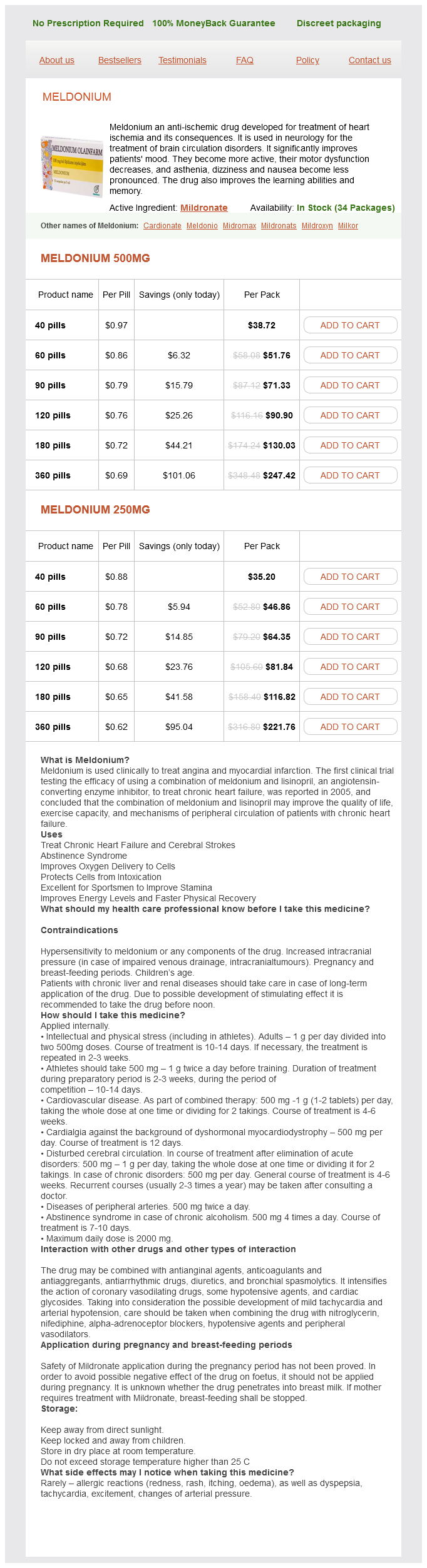
Meldonium 500mg
- 40 pills - $38.72
- 60 pills - $51.76
- 90 pills - $71.33
- 120 pills - $90.90
- 180 pills - $130.03
- 360 pills - $247.42
Meldonium 250mg
- 40 pills - $35.20
- 60 pills - $46.86
- 90 pills - $64.35
- 120 pills - $81.84
- 180 pills - $116.82
- 360 pills - $221.76
Therapeutic calcium alone has been associated with increased risks of myocardial infarction administering medications 7th edition quality mildronate 250 mg. Vitamin D supplementation alone can prevent falls in over-60-year-olds living in institutionalised settings or the community. Colecalciferol (vitamin D3) oral preparations are available as single agents or in combination with calcium in various formulations. Those exceeding the therapeutic threshold should be treated and those below given lifestyle advice and reassessed after 5 years, or sooner as required. Premenopausal women and those under 50 who have had an osteoporotic fracture should be referred for specialist management. The choice of drug will depend on cost-effectiveness, drug safety profile and patient factors, such as comorbidities, preferences, ability to comply with administration instructions and tolerance. Risedronate, if alendronate cannot be tolerated, adhered to or is contraindicated. The use of strontium ranelate is now restricted to severe osteoporosis when other drugs cannot be used and in those without cardiovascular contraindications. Poor adherence and persistence with oral bisphosphonates is a real problem, particularly within 3 months of initiation, as the risk of fractures increases when adherence falls below 50%. For those on oral bisphosphonates, explain that these must be taken whole on an empty stomach with a full glass of water and the patient must remain upright for 30 minutes after taking the medication to improve absorption and reduce the risks of oesophageal reactions. Explain duration of treatment and that the outcome is only to reduce the risk, not completely eliminate fractures. Osteoporosis 307 Explain common and severe adverse drug effects, including what signs to look out for and actions to take. Explain the need to maintain good oral hygiene, regular dental check-ups and timing of dental procedures for those taking bisphosphonates. Explain complex dosing instructions clearly to reduce the risks of adverse effects, especially around the time the drug is initiated. Alendronate, etidronate, risedronate, raloxifene, strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended). Alendronate, etidronate, risedronate, raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended). Strontium ranelate: cardiovascular risk restricted indication and new monitoring requirements. Various devices are used for the delivery of oxygen to the patient, usually via a pressure regulator and flow meter, which control the high pressure of oxygen delivered from the cylinder or other source. O Nasal cannulae or simple facemasks generally deliver a higher concentration of oxygen as flow rate is increased. Nasal cannulae are generally preferred by patients as they are comfortable and allow patients to eat while in situ. Non-rebreathing or reservoir masks are used to deliver higher concentrations of oxygen (60 80% or above) in acute situations. Venturi masks deliver a constant oxygen concentration within and between breaths (increasing flow does not increase oxygen concentration). Oxygen therapy can be used in acute situations where there is hypoxia because of reduced ventilation or acute lung injury, when there is underlying chronic lung disease or when it is important to maintain oxygen delivery to tissues. Oxygen should be prescribed to achieve a target saturation of 94 98% for most acutely ill patients or 88 92% for those at risk of hypercapnic (type 2) respiratory failure. However, few patients benefit from this and such therapy should only be given if assessed formally. Please use my % Venturi mask to achieve an oxygen saturation of % to % during exacerbations. Correction of hypoxia may have other benefits, such as reducing polycythaemia, and reducing or preventing progression of pulmonary hypertension. Chronic Obstructive Pulmonary Disease: Management of chronic obstructive pulmonary disease in adults in primary and secondary care (partial update). Acute pain is usually associated with tissue damage and healing, whereas chronic (persistent) pain is continuous, long-term pain of more than 12 weeks, or persisting after the time that healing should have occurred. Pain assessment Reliable assessment of pain is essential for both clinical trials and effective pain management. Chronic pain assessment requires assessment of the impact of pain on physical, emotional and social functions and requires multidimensional tools and health-related quality-of-life instruments. Acute pain must be assessed both at rest (important for comfort) and during movement (important for function and risk of postoperative complications). Some are disease-specific, such as the Western Ontario and MacMaster Universities for osteoarthritis, and others have more general application. Analgesic drugs may be prescribed regularly if the pain is continuous or when required if the pain is more variable. Regular reassessment is required to monitor effectiveness as analgesic requirements may change. The management of both acute and chronic pain requires a multidisciplinary approach including anaesthetists, nurses and pharmacists. Pain management services are usually led by an experienced clinician, often with access to appropriate physiotherapy and psychological treatments. Pain management 313 Pharmacological treatment options for pain Paracetamol Despite much investigation and being used for over 50 years, the mechanism of action for paracetamol remains unclear.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.