
Propranolol
General Information about Propranolol
While propranolol is usually well-tolerated, like several medication, it does come with potential unwanted effects. These may embrace dizziness, fatigue, and nausea. It is necessary to at all times comply with the dosage directions supplied by a healthcare professional and to report any unwanted effects experienced.
Propranolol is also commonly prescribed for people who've skilled a heart attack. By slowing down the center fee and reducing blood strain, this medication can help ease the pressure on the center and help within the recovery course of. It may be used to stop future heart attacks by bettering the heart's total operate and lowering the chance of abnormal coronary heart rhythms.
In addition to slowing down the center, propranolol additionally works by slowing sure impulses in the coronary heart. This is important because in some heart situations, there could additionally be abnormal electrical impulses that may cause the heart to beat too fast or too irregularly. By slowing these impulses, propranolol can help regulate the center's rhythm and forestall probably life-threatening arrhythmias.
Aside from its use in treating heart-related points, propranolol has additionally been found to be efficient in managing signs of tension. The treatment has a relaxing impact on the physique, which might help individuals who suffer from performance nervousness or social anxiety. It works by blocking the physical signs of anxiety, similar to a fast heartbeat and trembling, which might help individuals really feel more in control and fewer anxious in annoying situations.
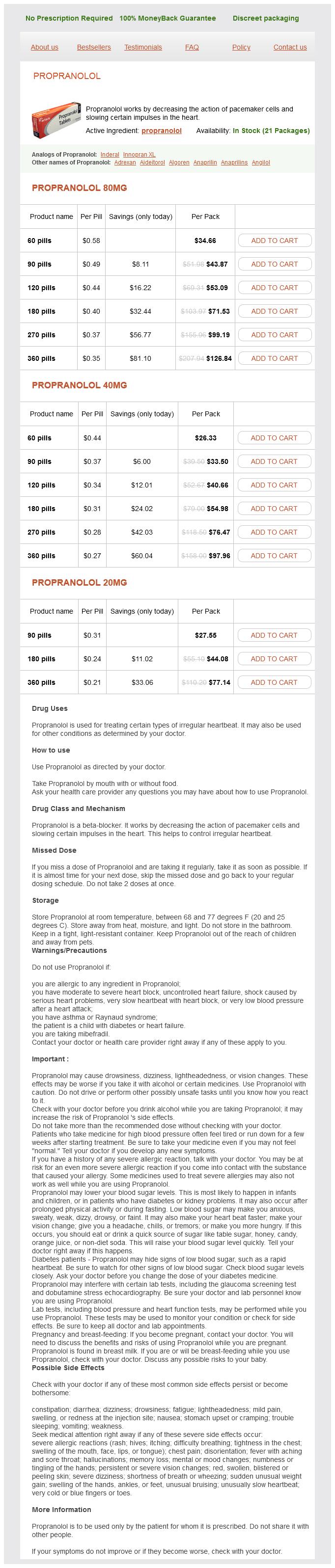
Propranolol is a medication that is commonly used to treat a selection of heart-related situations. It is a beta blocker, which signifies that it really works by blocking the effects of the hormone epinephrine on the body. This results in a lower in heart price and blood stress, making it an efficient remedy for circumstances such as high blood pressure, arrhythmias, and angina.
One of the important thing ways in which propranolol works is by lowering the motion of pacemaker cells within the heart. These cells are responsible for setting the rate and rhythm of the guts. When they are overactive, they will trigger a fast and irregular heartbeat, which can be harmful for people with certain heart circumstances. Propranolol blocks the receptors on these cells, inhibiting their activity and slowing down the heart rate.
In conclusion, propranolol is a commonly prescribed medication for quite lots of heart-related situations. By decreasing the action of pacemaker cells and slowing certain impulses in the coronary heart, it could successfully lower coronary heart price and blood strain, and enhance heart perform. It may be used to manage signs of hysteria. For individuals with heart points, propranolol can be a life-saving treatment, providing priceless support in sustaining a wholesome coronary heart rhythm and function.
Even with the presgroups reported some relief of neck pain and disability cardiovascular system as you age purchase propranolol paypal, measured using Neck Disability Index scores, and it was superior in the group receiving multimodal physical therapy (P=. However, the overall e ects of both programs were mitigated in the group presenting with both widespread mechanical and cold hyperalgesia. Further research aimed at testing the validity of this sub-group observation is warranted. A comprehensive review of the available scientific evidence produced a set of unambiguous patient centered messages that challenge unhelpful beliefs about whiplash, promoting an active approach to recovery. The use of this rigorously developed educational booklet (The Whiplash Book) was capable of improving beliefs about whiplash and its management for patients with whiplashassociated disorders. I 99 conducted a preliminary randomized A reduction in pain alone is not su cient to address the neuromuscular control deficits in patients with chronic symptoms, as these deficits require specific rehabilitation techniques. Support for specificity in rehabilitation can be indirectly found from a recent populationbased, incidence cohort study evaluating a government policy of funding community and hospital-based fitness training and multidisciplinary rehabilitation for whiplash. No supportive evidence was found for the e ectiveness of this general rehabilitation approach. Therefore, only addressing the lack of fitness and conditioning in this patient population may not be the most e cacious approach to treatment. One hundred twelve consecutive subjects were randomized to 1 of 2 treatment groups: educational intervention or usual care. The education intervention group received an educational pamphlet based on the current evidence, whereas the control group only received usual emergency department care and a standard non-directed discharge information sheet. Predictors of outcome following whiplash injury have been limited to socio-demographic and factors of symptom location and severity, which are not readily amenable to intervention. However, evidence exists to demonstrate that psychological factors are present soon following injury and play a role in recovery from whiplash injury. These factors can be as diverse as the physical presentation and can include a ective disturbances, anxiety, depression, and fear of movement. Recommendation: To improve the recovery in patients with whiplash-associated disorder, clinicians should (1) educate the patient that early return to normal, non-provocative pre-accident activities is important, and (2) provide reassurance to the patient that good prognosis and full recovery commonly occurs. A Neck Pain Impairment/Function-based Diagnosis, Examination and Intervention Recommended Classification Criteria* * Recommendation based on expert opinion. Levetiracetam is a white to off-white crystalline powder with a faint odor and a bitter taste. Inactive ingredients: ammonium glycyrrhizinate, citric acid monohydrate, glycerin, maltitol solution, methylparaben, potassium acesulfame, propylparaben, purified water, sodium citrate dihydrate and natural and artificial flavor. The antiepileptic activity of levetiracetam was assessed in a number of animal models of epileptic seizures. Levetiracetam did not inhibit single seizures induced by maximal stimulation with electrical current or different chemoconvulsants and showed only minimal activity in submaximal stimulation and in threshold tests. Protection was observed, however, against secondarily generalized activity from focal seizures induced by pilocarpine and kainic acid, two chemoconvulsants that induce seizures that mimic some features of human complex partial seizures with secondary generalization. Levetiracetam also displayed inhibitory properties in the kindling model in rats, another model of human complex partial seizures, both during kindling development and in the fully kindled state. The predictive value of these animal models for specific types of human epilepsy is uncertain. In vitro and in vivo recordings of epileptiform activity from the hippocampus have shown that levetiracetam inhibits burst firing without affecting normal neuronal excitability, suggesting that levetiracetam may selectively prevent hypersynchronization of epileptiform burst firing and propagation of seizure activity. A saturable and stereoselective neuronal binding site in rat brain tissue has been described for levetiracetam. Pharmacokinetics the pharmacokinetics of levetiracetam have been studied in healthy adult subjects, adults and pediatric patients with epilepsy, elderly subjects and subjects with renal and hepatic impairment. Overview Levetiracetam is rapidly and almost completely absorbed after oral administration. The pharmacokinetics are linear and Page 2 of 34 time-invariant, with low intra- and inter-subject variability. Levetiracetam is not significantly protein-bound (<10% bound) and its volume of distribution is close to the volume of intracellular and extracellular water. The major metabolic pathway of levetiracetam (24% of dose) is an enzymatic hydrolysis of the acetamide group. It is increased in the elderly (primarily due to impaired renal clearance) and in subjects with renal impairment. Absorption And Distribution Absorption of levetiracetam is rapid, with peak plasma concentrations occurring in about an hour following oral administration in fasted subjects. The oral bioavailability of levetiracetam tablets is 100% and the tablets and oral solution are bioequivalent in rate and extent of absorption. Food does not affect the extent of absorption of levetiracetam but it decreases Cmax by 20% and delays Tmax by 1. The pharmacokinetics of levetiracetam are linear over the dose range of 500 5000 mg. Levetiracetam and its major metabolite are less than 10% bound to plasma proteins; clinically significant interactions with other drugs through competition for protein binding sites are therefore unlikely. The major metabolic pathway is the enzymatic hydrolysis of the acetamide group, which produces the carboxylic acid metabolite, ucb L057 (24% of dose) and is not dependent on any liver cytochrome P450 isoenzymes. Two minor metabolites were identified as the product of hydroxylation of the 2-oxo-pyrrolidine ring (2% of dose) and opening of the 2 oxo-pyrrolidine ring in position 5 (1% of dose). There is no enantiomeric interconversion of levetiracetam or its major metabolite. Elimination Levetiracetam plasma half-life in adults is 7 ± 1 hour and is unaffected by either dose or repeated administration. Levetiracetam is eliminated from the systemic circulation by renal excretion as unchanged drug which represents 66% of administered dose.
Twelve of 14 patients had good loco-regional control in this study with short-term follow-up (mean 18 months) coronary heart bypass graft order propranolol without a prescription. A recent study retrospectively reviewed 25 patients who had 37 lymph nodes ablated between the years 1994-2012, with a relatively long follow-up of a mean of 65 months (879). Serum Tg levels were reduced in most patients and brought into an acceptable range (< 2. These investigators treated patients with only one session and 24% of patients had a recurrence at the site of the injection. Limitations of many of the studies included small numbers of patients, relatively shortterm follow-up, and many patients with small lymph nodes (<5-8 mm). More recently, preliminary findings using ultrasound guided laser ablation for treatment of cervical lymph node metastases have been reported (886). Efficacy has been suggested only in retrospective studies on limited numbers of patients (888;889). Likewise, systemic therapies (such as cytotoxic chemotherapy or kinase inhibitors) Thyroid Downloaded from online. Patient outcome is related to complete resection of all gross disease with the preservation of function, with techniques ranging from shaving tumor off the trachea or esophagus for superficial invasion, to more aggressive techniques when the trachea is more deeply invaded. Surgical decision-making can be complex and must balance oncologic surgical completeness with preservation of upper aerodigestive track head and neck function. In some circumstances such surgery represents a possible attempt for cure and in 216 Page 217 of 411 217 other circumstances offers significant regional neck palliation in patients with distant metastasis with impending asphyxiation or significant hemoptysis (414;891). However, there are no randomized, controlled clinical trials demonstrating better patient outcomes after radioiodine therapy. One retrospective analysis indicated that a delay in radioiodine therapy of six months or more was associated with disease progression and reduced survival (897). Despite the apparent effectiveness of 131 I therapy in many patients, the optimal therapeutic activity remains uncertain and controversial (895;899). There are three approaches to 131 I therapy: empiric fixed amounts, therapy determined by the upper limit of blood and body dosimetry (900;901)(902-907), and quantitative tumor or lesional dosimetry (908;909). Comparison of outcome among these methods from published series is difficult (895;897;900). No prospective randomized trial to address the optimal therapeutic approach has been published. One retrospective study concluded that patients with loco-regional disease were more likely to respond after dosimetric therapy than after empiric treatment (915). Another study demonstrated improved efficacy of administration of dosimetric maximal activity after failure of empiric dosage (916). Arguments in favor of higher activities cite a positive relationship between the total 131 I uptake per tumor mass and outcome (908), while others have not confirmed this 123 relationship (917). The radiosensitivity is higher in patients who are younger, with small metastases from well-differentiated papillary or follicular Thyroid Downloaded from online. These estimates imply the need for caution in administering empiric activities higher than 100-150 mCi in certain populations such as elderly patients and patients with renal insufficiency. Such patients should be given the same or higher activity that would have been given had they been prepared with hypothyroidism or a dosimetrically determined activity. With metastatic deposits in the brain or in close relation to the spinal cord or the superior vena cava, such swelling may severely compromise neurologic function or produce a superior vena cava syndrome, respectively. When detected, institution of temporary high dose 220 Page 221 of 411 221 corticosteroid therapy is recommended in an attempt to limit the risk of acute tumor swelling and compromised function. One study (940) found that 221 Page 222 of 411 222 lithium increased the estimated 131 I radiation dose in metastatic tumors on average by more than twofold, but primarily in those tumors that rapidly cleared iodine. Lithium use may be associated with adverse events and needs to be precisely managed. The overall approach to treatment of distant metastatic thyroid cancer is based upon the following observations and oncologic principles: 1. Morbidity and mortality are increased in patients with distant metastases, but individual prognosis depends upon factors including histology of the primary tumor, distribution and number of sites of metastasis. In the absence of demonstrated survival benefit, certain interventions can provide significant palliation or reduce morbidity (847;949-951). Longitudinal re-evaluation of patient status and continuing re-assessment of potential benefit and risk of intervention is required. However, evidence is currently insufficient to support a prognostic role of any specific gene testing for prognosis, and is absent to support selection of any specific therapy proven to enhance patient outcomes. Thus, routine mutation profiling cannot be recommended at this time outside of research settings. There is little if any benefit derived from the treatment of radioiodine refractory differentiated thyroid cancer with radioiodine (953). Pulmonary pneumonitis and fibrosis are rare complications of high-dose radioactive iodine treatment. Dosimetric approaches to therapy with a limit of 80 mCi whole-body retention at 48 hours and 200 cGy to the bone marrow should be considered in patients with diffuse 131 I pulmonary uptake (955). If pulmonary fibrosis is suspected, then 224 Page 225 of 411 225 appropriate periodic pulmonary function testing and consultation should be obtained. Other approaches (see sections C36-C41) should be considered once maximal cumulative tolerable radiation doses have been administered.
Propranolol Dosage and Price
Propranolol 80mg
- 60 pills - $34.66
- 90 pills - $43.87
- 120 pills - $53.09
- 180 pills - $71.53
- 270 pills - $99.19
- 360 pills - $126.84
Propranolol 40mg
- 60 pills - $26.33
- 90 pills - $33.50
- 120 pills - $40.66
- 180 pills - $54.98
- 270 pills - $76.47
- 360 pills - $97.96
Propranolol 20mg
- 90 pills - $27.55
- 180 pills - $44.08
- 360 pills - $77.14
While dissecting and removing the upper pole ureter cardiovascular system heart function order genuine propranolol on line, care should be taken to not damage the blood supply to the lower pole ureter. The ureterocele should be aspirated through the upper pole ureter at the end of the procedure. With this procedure, the excised upper pole moiety and ureter can be removed through the same incision. The risk of the need for further intervention is increased by ectopic ureterocele (reoperation risk of 65 percent) and high-grade reflux into another moiety (5070 percent reoperation rate). There is a 15 percent risk of requiring reoperation, but also a risk of damage to the sphincter mechanism when an ectopic ureterocele is enucleated. There is a reoperation rate for continuing reflux into the lower pole ureter, or into the upper pole stump. This procedure is performed through a small inguinal incision and musclesplitting approach allowing access to the retroperitoneal space. Both ureters are identified, the upper pole ureter is transected and the remaining distal upper pole ureter removed to the level of the sphincter. Care must be taken with extravesical extension, as this can lead to damage of the sphincter mechanism. This procedure, described above, is performed using an extraperitoneal groin incision. Care must be taken to reimplant double ureters en bloc, otherwise the shared blood supply associated with the common sheath will be impaired. At some institutions, either sub- or intraureteric injection of a bulking agent (see Chapter 84) is being used instead of a ureteric reimplantation. If performed laparoscopically, the kidney may be approached transperitoneally or retroperitoneally. Duplex kidneys: a correlation with renal dysplasia with position of the ureteric orifice. Incontinent diversions entail cutaneous drainage of urine into a pad, nappy, or stoma bag. Attention should also be directed toward the nutritional status, cardiovascular status, and neurological status of the child. Assessment by the anesthetist well in advance of surgery may be advisable in complicated cases. Before a decision can be made regarding the appropriate procedure for a particular child, the capabilities, compliance, and circumstances of the child and carers must be taken into consideration. In cases of posterior urethral valves, although primary fulguration is the ideal method of treatment, we have found there to be no difference in the outcome for boys with posterior urethral valves who had an initial vesicostomy and delayed ablation as compared to primary fulguration. Vesicostomy has a high incidence of stomal stenosis and prolapse in the long term and should not be considered as a permanent option. Incision 1a Urachal ligament Peritoneum 1b,c A short transverse incision a few centimeters in length is made above the pubic symphysis in an area that will drain into the pad/nappy. We have used this method in selected children under one year of age with solitary kidneys and a ureterovesical junction obstruction with deteriorating renal function. The site of the incision is modified depending on the site of the intended diversion; however, the approach to the ureter remains extraperitoneal. The ureter is identified by dividing the obliterated umbilical artery (illustration b). In cases of dilated tortuous and adynamic upper tracts, good drainage may not be achieved with a ureterostomy and an indwelling catheter or intermittent catheterization of the stoma may be necessary. However, in very carefully selected cases, this may be a useful option, for example in children with neuropathic bladder or pelvic malignancy who, along with their carers, may prefer this to major urinary tract reconstruction and continent diversion in the short to medium term. Incision the ileum can be approached through the same incision as that for the primary procedure if the diversion is being performed concomitantly. Ileal conduit Because of the high incidence of complications, an ileal conduit diversion is very uncommon nowadays in children. The distal end of the ileal loop is brought out at a suitable premarked position in the right iliac fossa and everted to create a nipple (illustration c). Two 4- or 6-Fr feeding tubes are left indwelling within the implanted ureters and exiting via the stoma. Problems with ureteral stenosis or vesicoureteric reflux may occur along with deterioration of renal function. CompliCations these are similar to those of an ileal conduit and include ureteral stenosis and kinking and deterioration of the upper tracts. A bladder outlet procedure may be performed simultaneously to increase outlet resistance. If an appendicovesicostomy is to be performed, mobilization of the appendix and mesentery can be performed at this stage. The peritoneum is closed, thereby extraperitonealizing the segment of ileum and bladder. The appendix is reimplanted in the bladder at this stage and a clam cystoplasty is performed with continuous 3/0 absorbable suture (illustration d). If an appendicovesicostomy has been created, an indwelling catheter is left within this conduit. In this case, the ileal patch may be reconfigured as a pouch (illustrations eg), which can be sutured to the bladder remnant. This principle was utilized by Mitrofanoff in 1980 to create a continent, catheterizable appendicovesicostomy.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.