
Renagel
General Information about Renagel
In conclusion, Renagel is an essential medication for patients with continual kidney illness on dialysis. It helps to cut back the amount of phosphorus within the blood, which is crucial for managing the condition and preventing complications. However, it's critical to take the treatment as prescribed and to tell the doctor of any unwanted effects or potential interactions with other medications. With proper use, Renagel may be an effective device in enhancing the standard of life for people with continual kidney disease.
Renagel comes in the form of oral tablets which might be taken with meals. The dosage and frequency of use could differ depending on the individual's situation and response to treatment. It is important to comply with the doctor's instructions and to not regulate the dosage with out medical recommendation.
One of some great benefits of Renagel is that it does not include calcium, unlike different phosphate binders, making it appropriate for patients who cannot tolerate calcium-based treatment. Additionally, it has a lower threat of side effects, such as gastrointestinal issues, in comparison with other phosphate binders.
However, like several medication, Renagel just isn't without its unwanted effects. The most typical ones embody constipation, diarrhea, nausea, and vomiting. These unwanted facet effects could additionally be managed by adjusting the dosage or taking the medicine with ample amounts of water. In rare circumstances, extra severe unwanted effects corresponding to issue respiratory and allergic reactions could occur, and medical attention must be sought immediately.
The use of Renagel is particularly for patients with continual kidney illness who are on dialysis. This is as a outcome of dialysis removes waste merchandise, including phosphorus, from the blood. However, the method isn't 100% environment friendly, and a few phosphorus may still be left in the blood after dialysis. Renagel helps to additional lower the phosphorus ranges in the blood and scale back the danger of complications.
Renagel, additionally known by its generic name sevelamer, is a drugs that is used for reducing the level of phosphorus within the blood in patients with chronic kidney disease who're on dialysis. It belongs to a category of medicine referred to as phosphate binders, which work by binding to dietary phosphorus within the digestive tract and stopping its absorption into the blood.
Renagel has also been found to interact with other medicines, so it is crucial to inform the doctor about all of the medications and dietary supplements being taken. This includes over-the-counter drugs, natural products, and vitamins.
Phosphorus is a mineral that's important for sustaining wholesome bones and enamel, however it can be dangerous when its ranges are too high within the blood. For people with continual kidney disease, the kidneys are unable to filter out extra phosphorus, resulting in a condition known as hyperphosphatemia. This could cause numerous complications similar to bone illness, heart illness, and even death. To help handle this situation, doctors might prescribe a medicine referred to as Renagel.
Omphalocele is characterized by herniation of abdominal contents through a defect chronic gastritis yahoo answers renagel 400 mg order with mastercard, although they are protected from the environment by a membrane. Omphalocele is associated with other anomalies including pentalogy of Cantrell, bladder or cloacal exstrophy, trisomy 21 (Down syndrome), or Beckwith-Wiedemann syndrome (15). Both gastroschisis and omphaloceles require surgical management, which typically involves gradual reduction of the externalized abdominal contents via a mesh or silo. The process can be performed through various procedures to allow for gradual expansion of the abdominal cavity. It can be complicated by abdominal competition and difficulty with ventilation due to increased intrathoracic pressures from a bulging diaphragm. Scoliosis Children may present for surgical correction of scoliosis that results from neuromuscular defects with misalignment of the vertebral column or simply as "idiopathic" scoliosis (2). In severe cases, gross deformities of the chest and abdomen may result in thoracic insufficiency and impair lung development. Furthermore, some patients may suffer neurologic sequelae such as nerve compression, which manifests as weakness, and sensory defects depending on the affected area. Surgical correction of scoliosis in a growing child remains controversial and treatment alternatives vary by surgeon, patient age, and coexisting disease. Surgical options include posterior spine fusion and vertical expandable prosthetic titanium rib. Anesthetic management should be tailored to meet the monitoring needs, as neurophysiologic monitoring may be used to assist and provide safety in the surgical approach. Agents that may affect the quality of motor and somatosensory-evoked potentials should be avoided, including volatile anesthetics, nitrous oxide, and neuromuscular blockade. Total intravenous anesthesia with propofol infusion and opioid infusions such as fentanyl or remifentanil are commonly used. The surgical procedures may be associated with significant hemodynamic derangements, including massive hemorrhage, spinal shock, coagulopathy, and hypothermia. Furthermore, positioning the patient should be done carefully to avoid pressure on the eyes, shoulders, and genitals to minimize position-related complications. Postoperative visual loss is uncommon but devastating and may occur as a result of ischemic optic neuropathy associated with the long duration of surgery. Intraoperative management should place specific emphasis on adequate intravascular access, with consideration for continuous arterial blood pressure monitoring as well as central venous access on a case-by-case basis. Blood conservation strategies such as antifibrinolytic agents, blood salvage techniques, and autologous blood donation may be used based on 648 Clinical Anesthesia Fundamentals the resources available. Postoperative Apnea Infants and neonates born preterm are at increased risk for postoperative apnea Hemodynamics Did You Know Children at risk for postoperative apnea should be admitted and observed on a ward with cardiorespiratory monitoring. In addition to prematurity, a history of apnea and anemia are risk factors for postoperative apnea. Intravenous caffeine may be administered and is effective in reducing the incidence of apnea, although postoperative admission is still warranted based on postconception age. Based on the available data, many institutions admit all former preterm infants until they reach an age of 60 weeks postconception age. Children with obstructive sleep apnea may be especially sensitive to respiratory depression associated with narcotics and general anesthesia. However, it is a significant concern and continues to be a cause of cardiac arrest in children (12). Treatment is with 100% oxygen, positive pressure, and maneuvers to ensure that upper airway obstruction is not present. Laryngospasm not relieved by these maneuvers should be treated with succinylcholine (22). If there are contraindications to succinylcholine, such as malignant hyperthermia or extensive burn injuries, a nondepolarizing neuromuscular blocking agent may be appropriate. Once desaturation has occurred, rapid neuromuscular blockade (succinylcholine) without delay is the treatment of choice. Secondary complications such as gastric insufflation, regurgitation, and aspiration can occur as a result of the sustained positive upper airway pressure that comprises appropriate management of laryngospasm. Postextubation Stridor Smaller children and infants are at increased risk for postextubation stridor due to their smaller diameter tracheas. More severe cases are treated with nebulized racemic epinephrine in addition to dexamethasone. Following treatment with racemic epinephrine, patients with improved symptoms should be observed for at least 4 hours to ensure rebound edema does not occur. Emergence Agitation or Delirium Emergence delirium is characterized by a state of delirium (confusion, lack of orientation to surroundings, agitation) in the immediate postoperative period following emergence from anesthesia (23). Since the introduction of sevoflurane into clinical practice, the incidence of emergence agitation has surged. Risk factors include young age (2 to 7 years), sevoflurane use, poor adaptability, and procedures near the face (ear, nose, throat, or ophthalmology). Emergence 33 Neonatal and Pediatric Anesthesia 649 agitation is a significant concern because agitated children can injure themselves, injure staff, or pull out catheters or drains and require additional staff to safely restrain and protect them. Most strategies have focused on prevention, and a variety of regimens are effective, including maintenance of anesthesia with propofol or intraoperative administration of dexmedetomidine, clonidine, and opioids. Initial management is typically observation and protection of the child from harm. More severe cases or prolonged cases may be managed with benzodiazepines, opioids, or subhypnotic doses of other sedatives. Indications and Contraindications In general, children presenting for outpatient procedures require being in optimal health and having no ongoing cardiorespiratory processes such as upper respiratory infections (1,2,5). Furthermore, the procedure must be amenable to pain control with medications administered by mouth. Although it is not necessary to demonstrate that a child is able to eat prior to discharge, the child should be willing and able to drink fluids and ensure he or she can take the necessary medications as indicated.
The three indications for elective revascularization procedures include claudication gastritis diet ������ order renagel on line, ischemic rest pain or ulceration, and gangrene. High-risk procedures, including ileofemoral bypass, femoral-femoral bypass, and aortofemoral bypass, re-establish blood flow to an ischemic extremity and relieve debilitating symptoms of claudication. However, advances in minimally invasive percutaneous techniques have made endovascular procedures the primary modality for revascularization. Regional or local anesthesia with or without sedation is often used for endovascular approaches. However, tunneling the graft and deployment of the stent can be quite painful and trigger patient movement or hypertension and tachycardia. Heparin is given prior to deployment of grafts or stents and anticoagulation may be needed in the postoperative period to maintain graft patency. Management strategies for asymptomatic carotid stenosis: A systematic review and meta-analysis. Open versus endovascular repair of abdominal aortic aneurysm in the elective and emergent setting in a pooled population of 37,781 patients: A systematic review and metaanalysis. Atherosclerosis occurs in two stages, the first is endothelial injury and the second is: A. How long should elective surgery be delayed after placement of a drug-eluting coronary stent The risk of cardiac-related death or nonfatal myocardial infarction after carotid endarterectomy is less than: A. Signs and symptoms of cerebral hyperperfusion syndrome after carotid endarterectomy include headache, seizures, and: A. Did You Know When chronic pain is associated with neuroplastic changes in the central and peripheral nervous systems that may manifest as hypersensitivity, windup, and allodynia, the pain itself becomes a disease state. Acute pain is a normal physiologic response to injury, disease, or surgery and is usually temporally self-limited. Though unpleasant, pain is protective and serves the purpose of avoiding, stopping, or minimizing tissue damage and should be seen as a symptom of an underlying disease. It can be due to ongoing disease or tissue injury or can persist after resolution of or in the absence of injury. Chronic pain is associated with neuroplastic changes in the central and peripheral nervous systems that may manifest as hypersensitivity, windup, and allodynia. Nociceptive pain results from transmission of a noxious stimulus through an intact nervous system. Nociceptive pain can be worsened by inflammation, which causes hyperalgesia, the phenomenon of normally painful stimuli being perceived as more painful than usual. Somatic pain originates within the skin, superficial tissue, and musculoskeletal system and is typically easy to localize and described as sharp. Visceral pain is typically vague, diffuse, achy, and may refer to surrounding areas. In contrast to nociceptive pain, neuropathic pain results from a lesion in the central or peripheral nervous system. Allodynia is the perception of pain from a normally nonpainful stimulus (such as light touch). Hyperesthesia is increased sensitivity to stimulation, and hypoesthesia is decreased sensation of stimulus. Pain Processing the physiology of pain processing functionally comprises four steps: transduction, transmission, modulation, and perception. These processes are clinically relevant as each provides targets for pain treatment and prevention. Transduction is the generation of an action potential from a noxious chemical, mechanical, or thermal stimulus. Transmission is the propagation of the signal through the afferent pathway from the nociceptor to the sensory cortex. Modulation is the positive or negative modification of the pain signal along the afferent pathway, while perception is the integration of the pain signal into consciousness. Transduction Nociceptors are located in the skin, mucosa, muscle, fascia, joint capsules, dura, viscera, and adventitia of blood vessels. When they are activated by pressure, chemical, or thermal stimuli, the channels activate voltage-sensitive sodium and calcium channels, starting an action potential. Nociceptors can be activated by bradykinin, serotonin, and protons and sensitized by prostaglandins, leukotrienes, and cytokines. Glutamate, substance P, and nerve growth factor can also promote transduction of a pain signal (Table 37-1). Transmission Pain transmission occurs via a three-neuron afferent pathway, beginning in the periphery. Fibers enter the spinal cord and travel up or down through the posterolateral tract before entering the dorsal horn to synapse on secondorder neurons. Second-order neuron cell bodies are located in the dorsal horn and are either nociceptive specific or wide dynamic range. Axons transmitting somatic nociception decussate and ascend via the contralateral spinothalamic tract, while axons transmitting visceral nociception ascend via the ipsilateral dorsal column medial lemniscus. Both synapse on the third-order neurons in the thalamus, the axons of which terminate in the sensory cortex. In the face, the primary afferent neuron has its cell body in the trigeminal ganglion and synapses on the second-order neuron in the medulla in the spinal trigeminal nucleus. From here the signal is transmitted to the thalamus, as are pain signals from the rest of the body. Modulation Modulation of the pain response occurs at many levels and can be positive or negative.
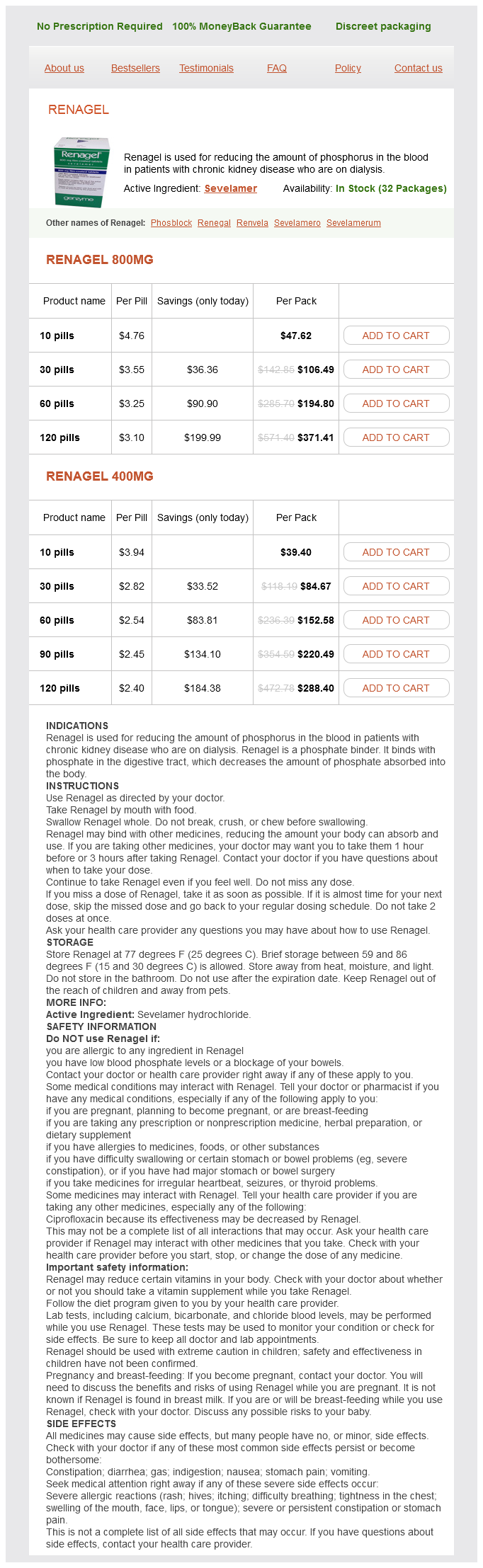
Renagel Dosage and Price
Renagel 800mg
- 10 pills - $47.62
- 30 pills - $106.49
- 60 pills - $194.80
- 120 pills - $371.41
Renagel 400mg
- 10 pills - $39.40
- 30 pills - $84.67
- 60 pills - $152.58
- 90 pills - $220.49
- 120 pills - $288.40
Such an anomaly is present in about 1 in 300 male newborns gastritis diet ���������� cheap 800 mg renagel with mastercard, but it can lead to problems with urination and ejaculation. Constriction of the opening may be present, increasing the risk for urinary tract infections. Infectious agents driving this process include Candida albicans, Gardnerella species, and pyogenic bacteria such as Staphylococcus aureus. Accumulated smegma (desquamated squamous epithelial cells and debris) beneath the foreskin predisposes to infection. Persistence of this inflammatory process predisposes to phimosis, a condition in which the prepuce cannot be retracted. This process is initially painless, but larger lesions may have erythema, ulceration, or crusting. The term erythroplasia of Queyrat is reserved for carcinoma in situ of mucosal surfaces (glans or prepuce). Bowenoid papulosis appears in younger patients as multiple, reddish brown papular lesions. Microscopically, all these lesions have dysplastic squamous cells involving the full epithelial thickness without invasion through the basement membrane. Such lesions are strongly associated with human papillomavirus infection, particularly types 16 and 18. Other factors, such as a history of smoking and lack of circumcision, are also implicated. When metastases occur, local inguinal and iliac lymph nodes are most often involved. Similar to cervical cancer in women, penile carcinoma is most often correlated with human papillomavirus infection, and the same types (16 and 18) are the most aggressive. Phimosis with increased accumulation of smegma is another risk factor; the incidence of penile cancer is rare in circumcised males. This form of cancer is often slow growing and locally invasive, but metastases can occur if left untreated. Note the extensive keratinization at low magnification in the left panel and well-differentiated cells at higher magnification in the right panel. Also known as the BuschkeLöwenstein tumor, it is typically a large, exophytic, cauliflower-like lesion of the genital or perianal area, with nonhealing ulceration and sometimes fistulas and sinuses. It arises most often in men and immunocompromised patients, usually on the glans penis of uncircumcised men. A similar verrucous gross and histologic appearance of squamous cell carcinoma may be seen in the oral cavity, larynx, skin of the soles, and anal region. Note the presence of two vestigial structures, the appendix testis and the appendix epididymis. The normal testis descends down into the lower abdomen under the influence of müllerian inhibiting substance. Final descent into the scrotum in the third trimester of fetal development occurs under the influence of increasing androgens. The Leydig cells of a cryptorchid testis function normally, but the increased body temperature diminishes spermatogenesis. Sertoli cells (or nurse cells) are inconspicuous because their attenuated cytoplasm interdigitates with the germ cells. Small dark oblong spermatozoa are visible in the center of the tubules because there is active spermatogenesis. Small nodular collections of pink Leydig cells are present in the interstitium between the tubules, secreting testosterone under the influence of luteinizing hormone. Note the pale golden-brown pigment in the interstitium, which gives the testicular parenchyma its grossly pale brown color. Sertoli cells secrete inhibin, which feeds back on the adenohypophysis to inhibit release of follicle-stimulating hormone, thus driving spermatogenesis. This left testis did not descend into the scrotum during fetal development, but remained in the abdomen, a condition known as cryptorchidism, which is unilateral in 75% of cases. The abnormal position causes no pain but predisposes to trauma, which does cause pain. A cryptorchid testis fails to develop normal spermatogenesis unless placed in the scrotum, because deterioration leading to the appearance shown begins by age 2. If unilateral, spermatogenesis in the remaining normal testis may prevent infertility. Cryptorchidism carries an increased risk for testicular carcinoma in either testis. Bilateral atrophy may occur with various conditions, including chronic alcoholism, hypopituitarism, atherosclerosis, chemotherapy or radiation therapy, and severe prolonged illness. Mumps, the most common infectious cause of orchitis, usually has a patchy and bilateral pattern of involvement that decreases the sperm count but does not usually lead to sterility. Mumps virus infection may be complicated by orchitis in one fourth to one third of cases. In general, the orchitis is unilateral and patchy, so sterility after infection is uncommon. Other infectious causes of orchitis include echovirus, lymphocytic choriomeningitis virus, influenza virus, coxsackievirus, and arboviruses. In contrast, epididymitis is a more frequent cause of scrotal pain and swelling in men and is most likely to be the result of a sexually transmissible disease, such as Chlamydia trachomatis or Neisseria gonorrhoeae in younger men or gram-negative bacteria from urinary tract infection in older men.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.