
Sildigra
General Information about Sildigra
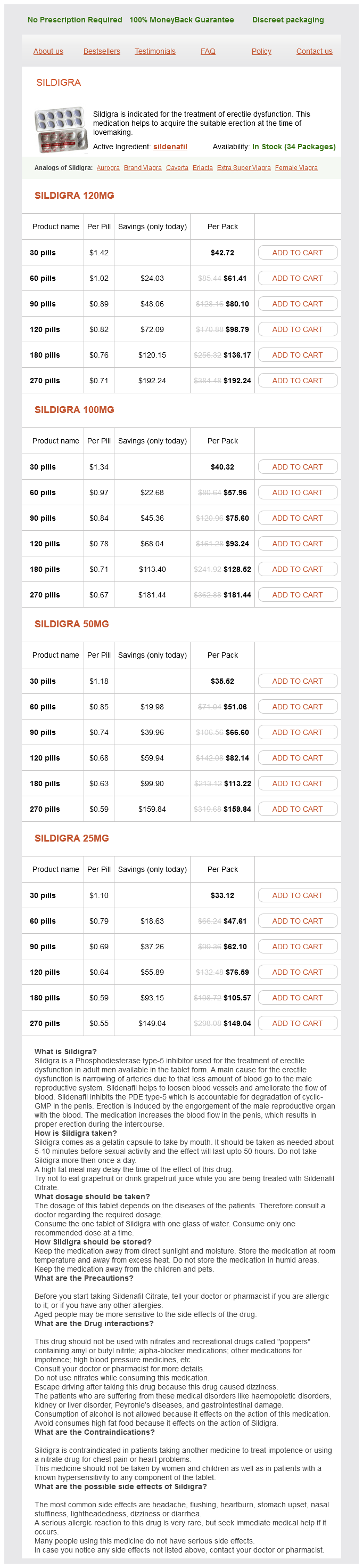
This treatment is normally out there in the type of oral tablets, with dosages ranging from 25mg to 100mg. It is essential to follow the prescribed dosage by your physician as it might vary relying in your specific condition. Sildigra should be taken roughly one hour earlier than sexual exercise and may be effective for up to four hours.
It is also crucial to note that Sildigra shouldn't be taken with certain drugs, similar to nitrates, as this can cause a harmful drop in blood stress. It is important to inform your doctor of any other medicines you're taking to ensure the safety and effectiveness of Sildigra for you.
As with any medicine, there could also be some potential unwanted aspect effects associated with Sildigra. These embrace complications, flushing, dizziness, nausea, and blurred vision. However, these unwanted aspect effects are usually mild and don't final lengthy. It is necessary to comply with the really helpful dosage and consult your doctor when you experience any persistent or extreme unwanted side effects.
Erectile dysfunction (ED) is a typical condition that impacts men of all ages, inflicting problem in acquiring or sustaining an erection throughout sexual exercise. This can greatly impact the standard of life and intimate relationships. Fortunately, there are medications obtainable to help treat this situation, certainly one of which is Sildigra.
In conclusion, Sildigra is a confirmed and efficient remedy for erectile dysfunction. It has helped numerous males regain their sexual perform and improve their overall quality of life. If you would possibly be experiencing signs of ED, seek the assistance of your physician to see if Sildigra is the right treatment possibility for you. Remember to all the time observe the prescribed dosage and report any unwanted aspect effects to your doctor. With the assistance of Sildigra, you'll have the ability to as soon as once more have a fulfilling and satisfying sex life.
Sildigra, also referred to as Sildenafil Citrate, is a drugs designed to help with erectile dysfunction. It belongs to a category of medicine referred to as phosphodiesterase type 5 (PDE5) inhibitors, which work by increasing blood circulate to the penile area. This helps to attain and maintain an erection throughout sexual exercise.
Not only does Sildigra help with erectile dysfunction, but it could possibly even have a optimistic influence on shallowness and total well-being. ED can typically result in emotions of inadequacy and frustration, which may greatly have an result on a person's psychological health. By successfully treating the symptoms of ED, Sildigra can help enhance an individual's confidence and self-worth.
The security and efficacy of Sildigra have been demonstrated in several clinical trials. In one research, greater than 80% of males with ED reported an improvement of their capability to realize and preserve an erection after taking Sildigra. In one other examine, Sildigra was found to be effective in males with various underlying well being situations, such as diabetes, high cholesterol, and hypertension.
Articles of clothing that patients need to remove include belts erectile dysfunction rates order sildigra in united states online, steel-tipped shoes/boots, hairpins, metallic jewelry (including body-piercing jewelry), clothing that contain magnetic threading, zippers, and snaps. If unsure of the magnetic properties of an object, a small handheld magnet can be used to determine if the object has risk. It also allows for ideal breath-holding because the operator is beside the patient and directly observing the patient breathing. Finally, hand injection allows for earlier detection of contrast reactions compared to power injection because the operator is closer to the patient. This is accomplished through the shortening of the T1 (spin-lattice) relaxation times of protons within tissues. Gadolinium-based, iron-containing, and manganese-containing compounds are currently approved by the U. Also, it transiently binds to albumin, which enables it to function as a conventional extracellular agent. Mangafodipir trisodium is a positive contrast agent, like the gadolinium-based agents, but with less enhancement at clinical doses. These agents are rapidly excreted through the kidneys with an elimination half-life of 15 to 90 minutes in patients with normal renal function. After injection into a vein, most gadolinium-based contrast agents travel to the arterial circulation, leak through capillaries, and finally redistribute into extracellular spaces. Clinical features of the disease are fibrosis of skin and connective tissue throughout the body. Fibrosis may occur in internal organs, such as the heart, lungs, and esophagus, and may disrupt their normal function. Blood-Pool Contrast In addition to extracellular distribution, some gadoliniumbased contrast agents can have blood-pool (intravascular), tissue-specific, or intracellular distributions. This enables better visualization of veins, smaller vessels, and vessels with slow or complex flow. Bloodpool agents have the potential for perfusion imaging, detection of gastrointestinal bleeding and stent graft leaks, and tumor imaging by way of demonstrating angiogenesis. It binds noncovalently to plasma albumin, enabling the visualization of blood vessels. This can be difficult for patients with claustrophobia or who are otherwise anxious about being in an unfamiliar environment with noises. These patients will probably be able to cooperate with the scan if premedicated with benzodiazepines, such as diazepam or alprazolam. An effective dose for a typical adult patient is 5 to 10 mg of diazepam or 1 to 2 mg of alprazolam taken orally approximately 30 minutes before scanning. It offers high spatial resolution with a minimum of artifacts to accurately diagnose numerous vascular conditions. Multiple methods have been developed that estimate when the contrast is expected to arrive at the imaging site. The "best guess" technique is one method for estimating the arrival of contrast at the imaging site. Another method for estimating the arrival of contrast at the imaging site is the "test-bolus" technique. Image acquisition times can then be adjusted with this information with a few more seconds added because the full contrast volume is normally larger than the test bolus. Limitations of this method include an error from early signal peaking due to the small, short-duration test bolus. The test bolus can add to background signal during the actual scanning because it has enough time to spread to the extracellular space. Automatic triggering and fluoroscopic triggering are other methods for timing the contrast with image acquisition. Even slight respiratory motions can obscure images of the intricate vasculature in these regions. It is possible to observe a patient breathing at baseline to estimate how long he or she will be able to hold his or her breath. If a patient is breathing at a rate of over 30 breaths per minute with little or no pauses between breaths, he or she may not be able to suspend breathing at all. Even though most patients find it easiest to hold their breath at maximum inhalation, it is sometimes preferred for them to hold their breath at end exhalation. This increases reproducibility in terms of anatomic positioning, especially when multiple, successive breath-holds are required. There is a physiologic limit for how fast the veins will allow contrast to be injected. Fast scanning is needed for proper image detail in the appropriate phase for time-resolved techniques. Threedimensional methods yield higher spatial resolution with no slice misregistration and work well with low-resistance flow. For peripheral imaging, however, 2D methods are used because they work better with slower, high-resistance, pulsatile flow. This increases image contrast because there is more consistently reliable blood in flow. Conversely, they can produce destructive interference and appear artificially darker with the possible loss of anatomic detail. New coil designs and pulse sequences are being developed that minimize these effects of 3. The increase in energy, which ultimately becomes heat, can potentially have adverse health effects. Also, it is sensitive to eddy currents, partial volume averaging, and changes in the velocity and amount of blood flow, such as with variations in cardiac output. Additionally, by varying the time delay between tagging and imaging, perfusionlike images of the kidneys, lungs, and liver can be produced without the use of contrast.
The more severe the cellular damage impotence at 75 sildigra 120 mg low cost, the greater the microvascular changes and with death of tissue, microvascular flow ceases within a few hours-the no-reflow phenomenon. When muscle tissue death is uniform, as would follow tourniquet ischemia or limb replantation, little inflammatory response results. In most instances of reperfusion, which follows thrombotic or embolic occlusion, there will be a variable degree of ischemic damage in the zone where collateral blood flow is possible. The extent of this region will determine the magnitude of the inflammatory response, whether local or systemic. In such emergency cases, acute hemodialysis is the only lifesaving treatment option. Compartment syndrome requires urgent surgical fasciotomy to prevent compression of microcirculation, resulting in complete necrosis of the calf muscle. Critical Limb Ischemia Limb salvage rates following infrapopliteal intervention are exceeding 90% in most publications irrespective of the treatment modality used. In patients with chronic wounds, the clinical impact of revascularization in preventing amputation is hard to predict. These patients require a multidisciplinary approach including wound care specialists, podiatrists, plastic surgeons, and diabetologists. Restenosis and reocclusion rates of more than 60% are reported 3 months after balloon angioplasty of long diffuse lesions. No controlled data exist about the effect of highspeed rotational atherectomy in long diffuse lesions. Appropriate cardiologic tests are recommended at least once a year to exclude significant coronary artery disease. Critical Limb Ischemia Appropriate wound care is essential following the revascularization procedure. For those patients, life style modification and guidelines conform adjustment of risk factor treatment is an essential part of the treatment strategy. Early restenosis following balloon angioplasty is usually a result of early recoil or dissection and can be treated by a repeat balloon angioplasty, atherectomy, or stenting procedure. In early reocclusion, thrombus aspiration followed by balloon angioplasty might be indicated; atherectomy could result in distal thrombus migration. If angiography does not result in an early failure of the previous intervention but no progress in wound healing was noted, revascularization of an additional infrapopliteal artery should be considered. Typical restenosis requires, in most cases, more advanced techniques than a simple repeat balloon angioplasty. The final treatment option, if endovascular strategies repeatedly failed and if a distal vessel segment would be available for anastomosis, might be distal crural or pedal bypass surgery. Moreover, improvement of infrapopliteal outflow in conjunction with femoropopliteal inflow procedures might become standard of care if these procedures will result in sustained patency of both inflow and outflow procedures. The most relevant predictor for treatment success is still the operator experience. Thus, technically challenging interventions should be focused on experienced centers of excellence. In parallel, individual physician training in such experienced centers should be offered more frequently. A stepwise approach oriented on the clinical benefit of a first procedure is possible. Moreover, complete infrapopliteal revascularization procedures including the foot arteries are possible with endovascular approach, whereas a bypass reconstruction is mostly limited to one infrapopliteal vessel. If distal landing zones for bypass anastomosis are not affected by endovascular procedures, the option for surgical revascularization is still preserved in case of acute or late endovascular revascularization failure. Currently, only a few limitations exist for endovascular infrapopliteal interventions: the major limitation is the dependency on operator experience and the limited access to interventional tools in some institutions. Technically, major limitations are (1) missing outflow distal to an occluded vessel segment and (2) severe vessel calcification. Durability of the procedures is still a matter of concern; however, drug-eluting solutions might become a breakthrough in the near future. Whether these technical improvements can be translated in improved patient outcomes has still to be proven. Infrapopliteal transcatheter interventions for limb salvage in diabetic patients: importance of aggressive interventional approach and role of transcutaneous oximetry. Currently, no dedicated trial results are available comparing the clinical efficacy of medical therapy, endovascular therapy, and surgical therapy of infrapopliteal disease. Prospective trial of infrapopliteal artery balloon angioplasty for critical limb ischemia: angiographic and clinical results. Prospective study of 713 belowknee amputations for ischaemia and the effect of a prostacyclin analogue on healing. Limb-threatening ischemia in the medically compromised patient: amputation or revascularization The use of angioplasty, bypass surgery, and amputation in the management of peripheral vascular disease. High prevalence of peripheral arterial disease and comorbidity in 6,880 primary care patients: cross sectional study. Reduced primary patency rate in diabetic patients after percutaneous intervention results from more frequent presentation with limb-threatening ischemia. Endovascular therapy as the primary approach for limb salvage in patients with critical limb ischemia: experience with 443 infrapopliteal procedures.
Sildigra Dosage and Price
Sildigra 120mg
- 30 pills - $42.72
- 60 pills - $61.41
- 90 pills - $80.10
- 120 pills - $98.79
- 180 pills - $136.17
- 270 pills - $192.24
Sildigra 100mg
- 30 pills - $40.32
- 60 pills - $57.96
- 90 pills - $75.60
- 120 pills - $93.24
- 180 pills - $128.52
- 270 pills - $181.44
Sildigra 50mg
- 30 pills - $35.52
- 60 pills - $51.06
- 90 pills - $66.60
- 120 pills - $82.14
- 180 pills - $113.22
- 270 pills - $159.84
Sildigra 25mg
- 30 pills - $33.12
- 60 pills - $47.61
- 90 pills - $62.10
- 120 pills - $76.59
- 180 pills - $105.57
- 270 pills - $149.04
First erectile dysfunction treatment prostate cancer sildigra 120 mg buy cheap, the use of multiple agents will increase the tumor cell kill of a treatment regimen. Second, utilizing agents with different mechanisms of action increases the range of interactions between tumor cells and drug, thus enhancing the synergy of the chemotherapeutic agents and targeting the heterogeneity of a tumor. Third, combination chemotherapy may prevent or slow the development of drug resistance. Before their use in the treatment of cancer, alkylating agents were better known for their use as chemical warfare agents ("mustard gas") in World War I. The survivors of the exposure event, who had been submerged in nitrogen mustard-rich waters, experienced profound bone marrow suppression and lymph node shrinkage. This effect was later harnessed in an effort to develop similar agents that would be useful for treating cancerous overgrowth of lymphoid tissues. Concepts Behind Radiosensitization with Chemotherapy Chemotherapeutic drugs that are able to produce significant sensitization of tumor cells to radiation treatment are termed radiosensitizers. The combination of radiotherapy and chemotherapy involves the individual cytotoxic actions of each treatment modality as well as the interactions between them and is termed chemoradiation. Many agents used in chemoradiation therapy also interfere with cellular repair mechanisms. Nucleoside analogs, such as gemcitabine, potently inhibit repair of genomic damage induced by ionizing radiation. In addition, they are preferentially cytotoxic to proliferative cells, thus slowing cell repopulation following fractionated radiation therapy. Chemoradiation therapy is limited by its narrow therapeutic index and significant potential toxicity to normal tissues during treatment. Efforts are ongoing to develop more selective and effective chemotherapeutic agents as well as agents that protect normal tissues or selectively target molecular processes responsible for tumor radioresistance or chemoresistance. Despite this classification, their greatest cytotoxic effects are seen in rapidly dividing cells. Alkylating agents are often used in combination regimens with other chemotherapy agents, especially in the systemic treatment of hematologic malignancies. The dose-limiting toxicity for alkylating agents is generally myelosuppression that manifests as neutropenia. Alkylating agents are not commonly used in interventional radiology procedures at the time of this review. Platinum Salts Platinum derivatives were serendipitously discovered in the 1960s when it was observed that bacterial growth was inhibited following electrical current delivery to the media through platinum electrodes. The antiproliferative action was noted to be similar to that produced by alkylating agents and radiation. Platinum compounds cause apoptosis most readily in cells that are actively replicating and are thus relatively cellphase specific. Cisplatin is a highly toxic antineoplastic agent that can cause potentially severe adverse events including dose-limiting nausea and vomiting (acute and delayed), nephrotoxicity with electrolyte disturbances, myelosuppression, ototoxicity, and peripheral neuropathies. Other, less toxic platinums have been developed, but all platinum agents are not active in the same cancers. Cisplatin has shown superior efficacy in many tumor types and is, therefore, still considered a valuable platinum agent despite its significant toxicity profile. In addition, most adverse events can now be reasonably controlled with aggressive supportive care including antiemetics and aggressive hydration to prevent nephrotoxicity. Their potential to cause renal damage, ototoxicity, and nausea or vomiting is much less when compared to that of cisplatin in equivalent doses. In contrast to cisplatin, the dose-limiting toxicities for carboplatin and oxaliplatin are myelosuppression and neuropathies, respectively. Carboplatin is most commonly dosed according to the Calvert formula, a calculation that uses target area under the curve and renal function parameters to estimate the dose for individual patients. Antimetabolites Antimetabolites are structural analogs of naturally occurring physiologic molecules found in the body. Macromolecules that are formed following incorporation of antimetabolites are incapable of carrying out their intended physiologic functions, ultimately resulting in apoptotic cell death. The process is completed by thymidine phosphorylase, an enzyme found in much higher concentrations in tumor tissue than in normal tissue. Cytarabine and gemcitabine are antimetabolite drugs that are structurally related to one another. The reduced folate used in clinical practice to "rescue" normal cells is calcium leucovorin. Tumor cell death ensues when strand breaks cannot be repaired before cell division is attempted. Anthracyclines also undergo electron reduction, which produces highly reactive free-radical species. Although free-radical production is not a major mechanism for tumor destruction, it is a well-studied cause of anthracycline toxicity and is responsible for cardiac damage as well as extravasation injury. Etoposide and teniposide are semisynthetic podophyllotoxin derivatives that are synthesized from extracts of the mayapple or mandrake plant. Epipodophyllotoxins are not commonly used in interventional radiology procedures at this time. Antimicrotubule Agents Antimicrotubule agents bind to tubulin, the structural protein that polymerizes to form microtubules. Inhibiting the movement of microtubules interferes with the normal balance of tubulin assembly or disassembly during mitosis, ultimately resulting in apoptosis. They bind to tubulin, inhibiting its polymerization and formation of the mitotic spindle during mitosis. They also retain some activity during the quiescent portion of the cell cycle because microtubules are involved in intracellular transport processes that occur throughout all phases of cellular development. The dose-limiting toxicity of vincristine is a peripheral neuropathy that is common to all antimicrotubule agents because functional microtubules are required for intracellular axonal transport.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.