
Sumycin
General Information about Sumycin
Like all drugs, Sumycin could cause unwanted effects in some individuals. These could embrace nausea, vomiting, diarrhea, and lack of appetite. More severe side effects, corresponding to allergic reactions, severe complications, and vision changes, must be reported to a healthcare professional instantly.
Another generally handled condition with Sumycin is acne. Acne is a pores and skin situation brought on by an overabundance of micro organism on the skin’s floor, leading to inflammation and the formation of pimples and blackheads. Sumycin works by reducing the amount of bacteria on the skin, serving to to clear up existing pimples and forestall future breakouts. It is usually prescribed together with different acne drugs for optimum effectiveness.
Sumycin is a broad-spectrum antibiotic that's commonly used in the treatment of assorted bacterial infections. This treatment belongs to a class of antibiotics generally known as tetracyclines and works by inhibiting the growth and unfold of bacteria in the physique.
Sumycin may be used to treat different forms of bacterial infections, corresponding to respiratory infections, skin infections, and sure kinds of pneumonia. It has also been found to be effective in the remedy of Lyme illness, a bacterial an infection spread by tick bites.
One of the most typical makes use of of Sumycin is for the remedy of urinary tract infections (UTI). UTIs are attributable to micro organism getting into the urinary tract and multiplying, leading to signs corresponding to painful urination, frequent urge to urinate, and lower stomach ache. Sumycin is efficient in opposition to many types of bacteria commonly involved in UTIs and is often prescribed by healthcare professionals for its reliable and confirmed results.
Sumycin is out there in several varieties, including tablets, capsules, and an oral suspension. It is normally taken two to 4 times a day, depending on the severity of the an infection being treated. It is important to follow the prescribed dosage and finish the entire course of remedy, even when symptoms begin to improve. Stopping the medication too quickly could result in the bacteria creating resistance to the antibiotic and end in a relapse of the an infection.
Sumycin may interact with sure drugs and dietary supplements, so it is essential to inform your doctor or pharmacist of any other medicines you take earlier than beginning remedy with Sumycin.
In conclusion, Sumycin is a trusted and efficient antibiotic used in the remedy of a selection of bacterial infections. Its broad-spectrum capabilities, together with its confirmed monitor document, make it a popular choice amongst healthcare professionals. If you would possibly be experiencing symptoms of a bacterial an infection, seek the assistance of your physician to see if Sumycin will be the proper therapy option for you.
Gonorrhea and chlamydia are two sexually transmitted infections (STIs) that can be successfully handled with Sumycin. These infections are caused by bacteria that can affect the reproductive organs and result in severe issues if left untreated. Sumycin has proven great success in treating these infections and is usually prescribed in combination with other drugs to make sure full eradication of the micro organism.
Daunorubicin is metabolized in the liver antibiotics for uti cipro dosage purchase 250 mg sumycin with mastercard, with formation of one of its primary metabolites, daunorubicinol, which has antitumor activity. Cytarabine undergoes extensive metabolism, with approximately 70% of the drug being recovered in the urine as the uracil arabinoside (ara-U) metabolite. Hepatotoxic agents-Concomitant use with other hepatotoxic agents may increase the risk of hepatotoxicity. Has not been studied in patients with serum bilirubin levels > 3 mg/dL, and caution should be used in this setting. Has not been studied in patients with severe renal dysfunction or end-stage renal disease, and caution should be used in these settings. In the presence of mild or moderate infusion reactions, the rate of infusion should be interrupted or slowed, and symptoms should be treated appropriately. If severe or lifethreatening reactions occur, the drug should be discontinued permanently, the symptoms should be treated, and the patient closely monitored until all symptoms resolve. Use with caution in patients previously treated with radiation therapy, as daunorubicin can cause a radiation-recall skin reaction. Patients should be cautioned to avoid sun exposure and to wear sun protection when outside. Aberrantly silenced genes, such as tumor suppressor genes, are then reactivated and expressed. Precise route of elimination and metabolic fate of decitabine is not known in humans. One of the elimination pathways is via deamination by cytidine deaminase, found principally in the liver but also in plasma, granulocytes, intestinal epithelium, and peripheral tissues. Approximately 70%80% is eliminated in feces, while the remaining 20%30% is eliminated in urine. Serum testosterone levels decrease to castrate levels within 3 days of initiation of therapy. Local discomfort at the site of injection with erythema, swelling, and/or induration. Chemotherapeutic and Biologic Drugs 177 D · Upon release of diphtheria toxin into cytosol, cellular protein synthesis is inhibited, and cell death via apoptosis occurs. Volume of distribution is similar to that of circulating blood, and the initial distribution half-life is approximately 25 minutes. Low serum albumin levels place patient at increased risk for vascular leak syndrome. Patients should be monitored closely throughout the entire treatment, including vital signs, pre- and post-infusion weights, and evidence of peripheral edema. Myelosuppression is uncommon, with anemia occurring more frequently than neutropenia. Hepatotoxicity with elevations in serum transaminases and hypoalbuminemia (albumin < 2. Usually occurs during the first course and resolves within 2 weeks of stopping therapy. Normal dynamic process of microtubule network is inhibited, leading to inhibition of mitosis and cell division. Less than 10% is eliminated as the parent compound, with the majority being eliminated as metabolites. Renal clearance is relatively minor, with less than 10% of drug clearance via the kidneys. Hypersensitivity reactions with generalized skin rash, erythema, hypotension, dyspnea, and/or bronchospasm. Usually prevented by premedication with steroid; overall incidence decreased to less than 3%. Presents as weight gain, peripheral and/or generalized edema, pleural effusion, and ascites. Metabolized extensively in the liver to the active hydroxylated metabolite, doxorubicinol, as well as to inactive metabolites. Important to be able to distinguish between hemorrhagic cystitis and the normal red-orange urine observed with doxorubicin therapy. Avoid using veins over joints or in extremities with compromised venous and/or lymphatic drainage. Use of a central venous catheter is recommended for patients with difficult venous access and mandatory for prolonged infusions. Risk of cardiotoxicity is higher in patients > 70 years of age, in patients with prior history of hypertension or pre-existing heart disease, in patients previously treated with anthracyclines, or in patients with prior radiation therapy to the chest. Cumulative doses of > 450 mg/m2 are associated with increased risk for cardiotoxicity. Myelosuppression is dose-limiting with leukopenia more common than thrombocytopenia or anemia. In contrast to parent drug, doxorubicin, which has a large Vd (7001,100 L/m2), liposomal doxorubicin has a small Vd (2 L/m2). Infusions of liposomal doxorubicin should be given at an initial rate of 1 mg/min over a period of at least 30 minutes to avoid the risk of infusion-associated reactions, which is a black-box warning. In the event of such a reaction, with flushing, dyspnea, or facial swelling, the infusion should be stopped immediately. Risk of cardiotoxicity is increased at total cumulative doses of doxorubicin approaching 550 mg/m2. It is also higher in patients > 70 years of age, in patients with prior history of hypertension or pre-existing heart disease, in patients previously treated with anthracyclines, or in patients with prior radiation therapy to the chest. Patients should be warned about the potential for red-orange discoloration of urine for 12 days after drug administration. Chronic form results in a dose-dependent dilated cardiomyopathy associated with congestive heart failure.
Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new onset epilepsy report of the Therapeutics and Technology Assessment Subcommittee and Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society antibiotics for acne risks purchase sumycin from india. Uncontrolled epilepsy following discontinuation of antiepileptic drugs in seizure-free patients: A review of current clinical experience. Socioeconomic characteristics of childhood seizure disorders in the New Haven area: An epidemiologic study. Epileptic seizures epilepsy and risk factors: Experiences with an investigation in Martinique. Pharmacogenetic and enzyme induction/inhibition properties of antiepileptic drugs. Antiepileptic drug use of women with epilepsy and congenital malformations in offspring. Multicentre, double-blind, randomized, comparison between lamotrigine and carbamazepine in elderly patients with newly diagnosed epilepsy. New onset geriatric epilepsy, a randomized study of gabapentin, lamotrigine, and carbamazepine. An international multicenter randomized double-blind controlled trial of lamotrigine and sustained-release carbamazepine in the treatment of newly diagnosed epilepsy in the elderly. Formulate an initial treatment strategy for a patient in generalized convulsive status epilepticus. Describe adverse drug events associated with the pharmacotherapy of status epilepticus. Phase I During phase I, autonomic activity increases, resulting in hypertension, tachycardia, hyperglycemia, hyperthermia, sweating, and salivation. Increases in sympathetic and parasympathetic stimulation with muscle hypoxia can cause ventricular arrhythmias, severe acidosis, and rhabdomyolysis which can lead to hypotension, shock, hyperkalemia, and acute kidney injury. She was started on fosphenytoin for seizure prophylaxis upon admission along with her home medications. Her nurse reports that a few minutes ago she was alert and awake, but now she is unarousable and is having jerky, convulsive movements on both sides of her body. The doctor evaluates her and the jerky activity stops, but then starts again about 1 minute later. Clinical Presentation of Status Epilepticus General the patient may present with or without clinically noticeable seizure activity. Cerebral metabolic demand remains high; however, the body is unable to compensate, resulting in hypoglycemia, hyperthermia, respiratory failure, hypoxia, respiratory and metabolic acidosis, hyperkalemia, hyponatremia, and uremia. This will help guide therapy and clarify necessary laboratory and diagnostic tests. Twitching of the face, hands, or feet may be seen in these comatose patients with prolonged seizures. Physical Examination Once seizures are controlled, a neurologic exam should evaluate the level of consciousness (coma, lethargy, or somnolence), motor function and reflexes (rhythmic contractions, rigidity, spasms, or posturing), and pupillary response. They may also be hypertensive, tachycardic, febrile, and diaphoretic which resolve after seizure termination. A loss of bowel or bladder function, respiratory compromise, and nystagmus may also be observed. Serum drug levels should be obtained in an overdose situation to rule out toxicity. Albumin levels, renal and liver function tests should also be utilized to assess therapy. Metabolic acidosis may resolve on its own without treatment after termination of clinical seizure activity. After seizures stop, clinicians must identify and treat underlying causes of the seizures, such as toxins, hypoglycemia, or brain injury. Patients with known seizure disorders should be evaluated for abrupt cessation of their medications, noncompliance, or drug interactions. When treating patients on chronic benzodiazepine therapy, consider using higher doses to overcome tolerance. Diazepam and lorazepam should be diluted 1:1 with normal saline before parenteral administration via peripheral veins to avoid vascular irritation from the propylene glycol diluent. Doses are infused no faster than 50 mg/minute due to risks of hypotension or arrhythmias. Phenytoin should not be infused with other medications because of stability concerns (it is soluble in propylene glycol and compatible only in 0. Extravasation of phenytoin can cause local tissue discoloration, edema, pain, and sometimes necrosis (purple glove syndrome). Fosphenytoin Fosphenytoin is a water-soluble, phosphoester prodrug that is rapidly converted to phenytoin in the body. Paresthesias, especially around the lips and groin are common, but typically resolve within a few minutes and should not necessitate stopping the infusion. Phenobarbital If phenytoin or fosphenytoin fails to prevent seizure recurrence, phenobarbital can be considered. Doses can be given every 5 minutes until seizure activity stops or toxicities are seen (eg, respiratory depression). Diazepam can be administered as a rectal gel enabling nonmedical personnel to provide timely therapy at home or in public areas. Lorazepam Less lipophilic than diazepam, lorazepam has a longer redistribution half-life, resulting in longer duration of action and decreased need for repeated doses. Both lorazepam and diazepam are effective in stopping seizures,13 but lorazepam is currently preferred due to a longer duration of action. It can be redosed every 5 to 10 minutes (up to a maximum cumulative dose of 8 mg) until seizure activity stops or side effects such as respiratory depression occur. Midazolam Midazolam is water-soluble and can be administered intramuscularly,14 buccally,15,16 and nasally.
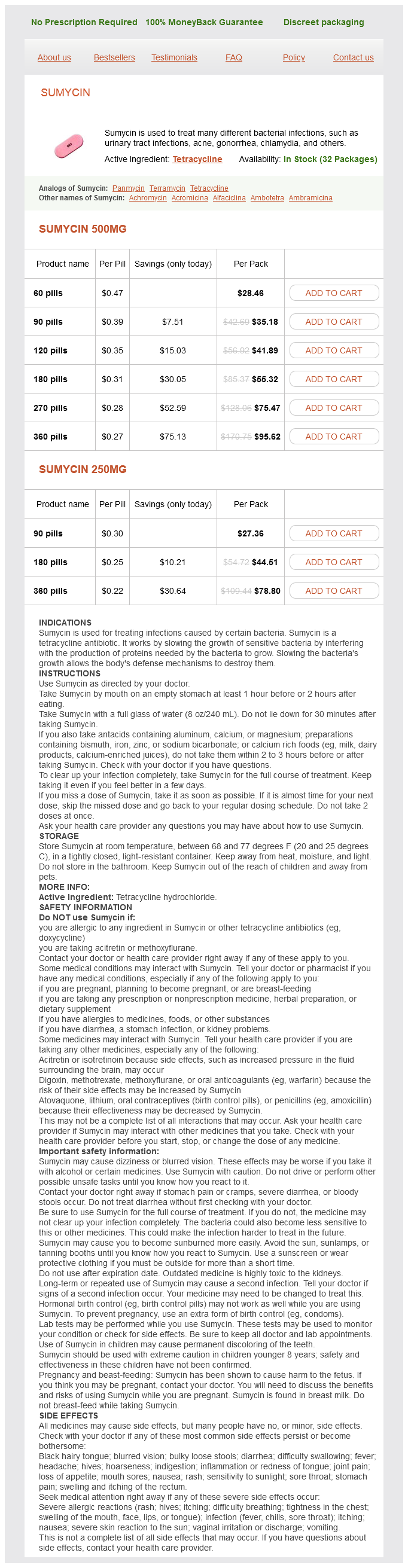
Sumycin Dosage and Price
Sumycin 500mg
- 60 pills - $28.46
- 90 pills - $35.18
- 120 pills - $41.89
- 180 pills - $55.32
- 270 pills - $75.47
- 360 pills - $95.62
Sumycin 250mg
- 90 pills - $27.36
- 180 pills - $44.51
- 360 pills - $78.80
Inadequate ultrafiltration and solute dialysis in patients with a large body size zinnat antibiotics for uti sumycin 250 mg buy low cost, unless large volumes and frequent exchanges are employed 5. Mechanical problems such as hernias, dialysate leaks, hemorrhoids, or back pain may occur 8. Advantages and disadvantages of hemodialysis and peritoneal dialysis are listed in Tables 269 and 2610, respectively. The dialyzer is composed of thousands of capillary fibers made up of the semipermeable membrane, which are enclosed in the dialyzer, to increase the surface area of blood exposure to maximize the efficiency of removing substances. The dialysate is composed of purified water and electrolytes, and it is run through the dialyzer countercurrent to the blood on the other side of the semipermeable membrane. The process allows for the removal of several substances from the bloodstream, including water, urea, creatinine, electrolytes, uremic toxins, and drugs. Sterilization is not required for dialysate because the membrane prevents bacteria from entering into the bloodstream. However, if the membrane ruptures during hemodialysis, infection becomes a major concern for the patient. Three types of membranes used for dialysis are classified by the size of the pores and the ability to remove solutes from the bloodstream: · Conventional (standard) membranes have small pores, which limit solute removal to relatively small molecules, such as creatinine and urea. An anticoagulant (usually heparin) is administered to prevent clotting in the dialyzer. The dialysate is pumped at the rate of 500 to 1000 mL/min through the dialyzer countercurrent to the flow of blood. The rate of fluid removal from the patient is controlled by adjusting the pressure in the dialysate compartment. At times, solutes can be added to the dialysate that are diffused into the bloodstream. Changing the composition of the dialysate allows for control of the amount of electrolytes that are being removed. Changing the hydrostatic Patient Encounter 4, Part 1 A 35-year-old Caucasian man with a history of IgA nephropathy presents to the clinic with complaints that he "feels awful. The catheters are tunneled beneath the skin to an exit site to reduce the risk of infection. Venous catheters can also be used as permanent access in patients in whom arteriovenous access cannot be established. Changing the pore size of the dialyzer membrane alters the efficiency of convection and allows for control of the amount of water removed in relation to the amount of solute being removed. The physiology of these complications is described below and the management is listed in Table 2611. It has been reported to occur with approximately 10% to 30% of dialysis sessions but may be as frequent as 50% of sessions in some patients. Hypotension associated with hemodialysis manifests as a symptomatic sudden drop of more than 30 mm Hg in mean arterial or systolic pressure or a systolic pressure drop to less than 90 mm Hg during the dialysis session. Ultrafiltration removes fluid from the plasma, which promotes redistribution of fluids from extracellular spaces into the plasma. However, decreased serum albumin levels and removal of solutes from the bloodstream decrease the osmotic pressure of the plasma relative to the extracellular spaces, slowing redistribution during hemodialysis. The predominant types of vascular access for chronic dialysis patients are (A) the arteriovenous fistula and (B) the synthetic arteriovenous forearm graft. The first primary arteriovenous fistula is usually created by the surgical anastomosis of the cephalic vein with the radial artery. The flow of blood may be diminished in the radial and ulnar arteries because it preferentially flows into the low pressure graft. The cause of infection is usually related to organisms found on the skin, namely Staphylococcus epidermidis and Staphylococcus aureus. The greatest risk to patients receiving hemodialysis is the development of bacteremia. Blood cultures should be obtained for any patient receiving hemodialysis who develops a fever. Nonpharmacologic management of infections involves preventive measures with sterile technique, proper disinfection, and minimizing the use and duration of venous catheters for hemodialysis access. Pharmacologic management of infections should cover the gram-positive organisms that most frequently cause accessrelated infections. Patients who have positive blood cultures should receive treatment tailored to the organism isolated. Preventive measures for access-related infections include mupirocin at the exit site and povidone-iodine ointment. Risk factors that may increase the potential for hypotension include elderly age, diabetes, autonomic neuropathy, uremia, and cardiac disease. Other contributing factors to the development of muscle cramps include hypotension and electrolyte and acidbase imbalances that occur during hemodialysis sessions. Thrombosis Thrombosis associated with hemodialysis most commonly occurs in patients with venous catheter access for dialysis and is a common cause of catheter failure. The vitamins that may require replacement are ascorbic acid, thiamine, biotin, folic acid, riboflavin, and pyridoxine. Patient Encounter 4, Part 2 the patient returns to the dialysis clinic 6 months later for his follow-up after starting peritoneal dialysis.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.