
Super Viagra
General Information about Super Viagra
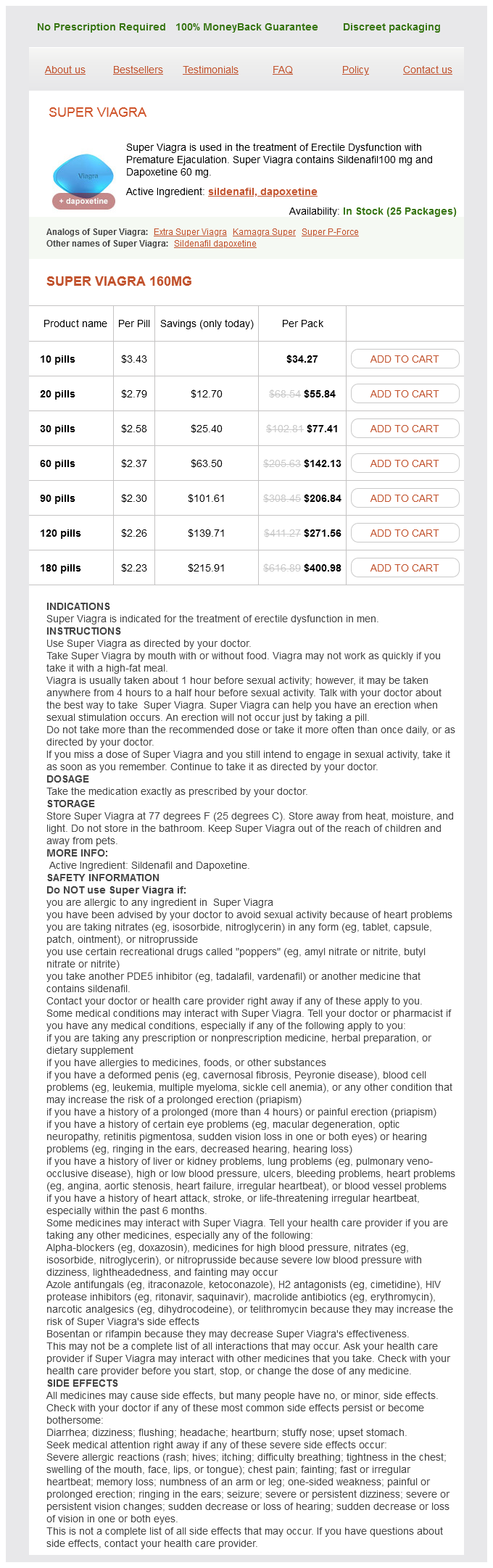
One of the significant advantages of Super Viagra is that it addresses both ED and PE simultaneously, making it a handy and cost-effective remedy choice for men that suffer from each conditions. It also reduces the need for males to take two separate drugs, as Super Viagra combines the benefits of both Sildenafil and Dapoxetine in a single pill.
Super Viagra comes in a tablet form and is usually taken orally, 30-60 minutes before sexual activity. It is crucial to note that Super Viagra isn't a remedy for ED or PE, and it only offers momentary reduction from the symptoms. It shouldn't be used as a leisure drug and should only be taken under the supervision and steering of a healthcare skilled.
The combination of these two elements in Super Viagra makes it a potent and efficient medication for men that suffer from both ED and PE. Sildenafil works by rising blood flow to the penis, allowing for a agency and lasting erection. Dapoxetine, however, works by delaying the ejaculation course of, helping men to have more control over when they climax.
Erectile dysfunction (ED) and premature ejaculation (PE) are two widespread sexual disorders that can have a big impression on a person's shallowness and quality of life. Many males who are suffering from one or both of these situations often feel embarrassed and ashamed, resulting in a reluctance to seek assist or discuss their issues with a healthcare skilled.
Fortunately, with the developments in modern medicine, there are now efficient remedy choices obtainable for both ED and PE. One such treatment that has gained reputation in latest times is Super Viagra.
As with any medicine, Super Viagra does have some potential unwanted aspect effects that customers ought to be aware of. These can include headaches, dizziness, nausea, flushing, and changes in vision. It is crucial to debate any underlying well being conditions or drugs with a physician earlier than starting Super Viagra, as it might interact with sure medications.
Super Viagra is a mix drug that's used within the remedy of ED with PE. It incorporates two lively elements: Sildenafil and Dapoxetine. Sildenafil is similar energetic ingredient found in the well-known ED medicine, Viagra, and is a phosphodiesterase sort 5 (PDE5) inhibitor. Dapoxetine is a selective serotonin reuptake inhibitor (SSRI) that's used specifically for the remedy of PE.
In conclusion, Super Viagra is a wonderful remedy possibility for males who struggle with each ED and PE. It offers the convenience of one tablet for both circumstances and has shown to be highly efficient in scientific trials. However, it's essential to consult with a healthcare professional before starting any new treatment, and to make use of Super Viagra as directed to see the best results. With Super Viagra, men can reclaim their confidence and luxuriate in a satisfying and wholesome intercourse life.
The freeze zone shown by intraoperative ultrasound closely approximates the pathologic and histologic volume of cryonecrosis erectile dysfunction treatment chennai super viagra 160 mg purchase line. Complete thawing of the tumor may take 20 to 30 minutes, extending the overall operative time. Because cryotherapy failure usually occurs at the periphery of the ice ball, it is necessary only to thaw the most peripheral centimeter of the ice ball before initiating the second freeze cycle; this reduces operative time without compromising clinical efficacy. After completion of the second freeze-thaw cycle, the probe is actively rewarmed, allowing it to disengage before the tumor completely thaws. The probe tract is packed with absorbable knitted fabric such as Surgicel or another hemostatic material, and gentle pressure is applied to the liver, preventing delayed hemorrhage from the probe tract. Rough handling of the thawing ice ball may cause a cleavage plane to develop at the interface of the ice ball and the normal liver parenchyma, which can cause massive bleeding. Generally, the probe insertion tract stops bleeding promptly as the coagulation cascade activates at body temperature. After the two freeze-thaw cycles, the treated volume usually remains hyperechoic on ultrasound, whereas the surrounding normal liver becomes hypoechoic because of edema. The reported experience with laparoscopic cryotherapy is scant, and the patients are highly selected. Studies have been limited to small case series (generally <10 patients), but the technique seems to be safe and effective in these highly select patients (Seifert & Junginger, 2004). Despite current technologic limitations, the advantages of the laparoscopic approach are that it is minimally invasive, it eliminates the morbidity associated with a laparotomy incision, and it decreases the length of hospitalization and overall recovery. This approach originally was limited by the large diameter of current cryoprobes, location of the tumors, and accurate radiologic localization. Despite these problems, several moderate-sized series have confirmed the feasiblity and safety of this approach. Fluid shifts tend to be minimal, and patients usually can be fed on postoperative day 2. There is usually a transient elevation of the liver enzymes, leukocytosis, decrease in platelet count, and fairly high fevers in the early postoperative period. The increase in liver transaminase levels is related directly to the volume of liver treated and usually resolves within 1 week. The platelet count falls for the first few days, then stabilizes, only to return to normal or supranormal levels in 7 to 10 days. Less frequently, the coagulation profile deteriorates with increased partial thromboplastin and prothrombin times, with elevation of serum levels of fibrin split products and D-dimer. Pleural effusions are common, as a result of liver mobilization and treatment of areas adjacent to the diaphragm. It is important that a reasonably standardized follow-up of patients, with careful documentation of recurrence patterns and disease-specific outcome, be collected on all patients. The patient should undergo clinical evaluation, serial liver tests, and tumor marker determinations every 3 to 4 months for 2 years and then every 6 months. Gas bubbles may be seen within the necrotic tumor and may be a result of the packed probe tract. These bubbles rarely indicate hepatic abscess and should not be acted on unless there are other signs of sepsis. In 3 to 6 months, the lesions shrink, leaving a persistent area of fibrosis and architectural distortion. The wire-guided Seldinger technique described earlier has been adapted to facilitate accurate placement of the laparoscopic cryoprobe. The dilators have been modified to make them stiffer than the dilators used in the open procedure. The probe is passed into the sheath, and the sheath is retracted to the liver edge during the freeze-thaw cycles. Some groups have used inflow occlusion with Pringle maneuver to diminish these effects. Experimental studies have not confirmed these assertions in the porcine model, in which clamping the hepatoduodenal ligament did not alter the size of the ice ball formed, the amount of liver necrosis, or the incidence of large-vessel infarction (Kahlenberg et al, 1998). Others have used thermocouples to monitor the temperature at the margin of the ice ball; however, this is an unnecessarily invasive procedure that provides no important additional information. Cracking the Ice Ball and Liver Surface Fracture Blood loss can be troublesome for patients undergoing cryoablation, especially for patients with cirrhosis with pancytopenia or thrombocytopenia. Bleeding can occur after a sizable freeze when a fair extension of the liver capsule is ablated. The capsule can crack when thawing, which leads to stellate fractures that can cause further bleeding. If these fractures are anatomically accessible, bleeding control is feasible to a certain degree during an operation, with sutures or hemostatic agents. In contrast, when fractures are located on the posterior surface of the liver, hemostasis can be more difficult to achieve due to lack of adequate exposure (McKinnon et al, 1996). Bile Duct Warming To protect the major bile ducts from the adverse effects of cryotherapy, some surgeons have cannulated the bile ducts to circulate warmed fluids during the cryoablation. The operative complications include complications that are not specific to cryotherapy, whereas the technical and late complications are directly related to the procedure (Table 98D. The overall morbidity rate ranges from 10% to 40%, and the mortality rate, 0% to 5% (Seifert & Junginger 2004). Myoglobinuria Acute kidney failure caused by myoglobin deposition in renal tubules can be a serious complication of cryoablation. The injury varies according to the amount of tissue that was frozen and the number of freeze-thaw cycles. In a series of 18 patients, there was an incidental finding of myoglobinemia and myoglobinuria (Onik et al, 1993).
Hollenberg Pharmacokinetics is the branch of pharmacology concerned with the movement and disposition of drugs within and by the body and includes drug absorption erectile dysfunction recreational drugs purchase super viagra toronto, distribution, metabolism, and elimination. Following administration, drugs are absorbed and distributed throughout the circulatory system to their sites of action. Most drugs are active in their administered form and are metabolized to inactive compounds, followed by elimination from the body; some drugs are metabolized to active compounds. Further, prodrugs are inactive in their administered forms and are metabolized to their active forms, typically followed by inactivation and elimination. This article discusses the absorption, distribution, metabolism, and elimination of drugs and the diverse factors that affect these processes. Drugs administered orally, intramuscularly, or subcutaneously must cross membranes to be absorbed and enter the systemic circulation. Drugs administered by intravenous injection must also cross capillary membranes to exit the systemic circulation and reach extracellular and intracellular sites of action. Even compounds whose actions are directed toward platelets or other blood-borne elements must cross membranes. Drugs that are uncharged, nonpolar, and have low molecular weight and high lipid solubility are easily transported across membranes. In contrast, drugs that are ionized or in which the electronic distribution is distorted, so that there is a separation of positive and negative charge imparting polarity, are not compatible with the uncharged nonpolar lipid environment. In addition, the ordered lipid membrane does not allow for the existence of aqueous pores large enough (>0. Large-molecular-weight proteins cannot pass through many membranes, and often, transmembrane transport of these moieties is an active process requiring energy and a carrier molecule. Lipid solubility or hydrophobicity is expressed as the oil/water equilibrium partition coefficient of a compound and is measured by determining the amount of a compound in each phase of an oil-H2O mixture following solubilization and attainment of equilibrium. Thus differences in absorption could be attributed solely to lipid solubility, and absorption was greatest for the barbiturate with the largest lipid solubility. This is critically important since how the body handles the drug plays a key role in determining the response of the individual to the drug. In nearly all cases, drugs must traverse membranes to reach their site(s) of action (Absorption). The drug then undergoes distribution to specific organs and tissues (Distribution). As part of absorption and distribution, the drug oftentimes undergoes enzymatic alteration of the chemical structure of the compound, leading to formation of a metabolite (or metabolites) (Metabolism). The drug and its metabolites are ultimately removed from the body by a variety of processes (Elimination). Numerous factors influence the rates of delivery, distribution, and disappearance of drug to and from its site of action. All of the processes and variables that influence the levels of a drug in the human body are described in this chapter. When planning drug therapy for a patient, deciding on the dosing schedule is critical to increase the effectiveness of the drug or to reduce symptoms of toxicity. In order to design an appropriate dosing schedule, several key pharmacokinetic parameters and principles must be understood. This article also describes the key pharmacokinetic concepts and parameters required for the rational design of dosing regimens. The circulatory system is the major pathway for drug delivery to its site of action. The compounds have roughly equivalent pKa values, so the degree of ionization is similar for all three drugs. An acid is defined as a compound that can dissociate and release a hydrogen ion, whereas a base can take up a hydrogen ion. The concentration gradient across the membrane is the driving force that establishes the rate of diffusion from high to low concentrations. It also assists in predicting which drugs will undergo tubular reabsorption, which is discussed later. In addition to simple passive diffusion, other mechanisms exist for transporting drugs across biological membranes, including active transport, facilitated diffusion, or pinocytosis. Active transport involves specific carrier molecules in the membrane that bind to and carry the drug across the lipid bilayer. Because there are a finite number of carrier molecules, they exhibit classical saturation kinetics. Drugs may also compete with a specific carrier molecule for transport, which can lead to drug-drug interactions that modify the time and intensity of action of a given drug. Further, because cellular energy is used to drive transport, an active transport system may concentrate a drug on one side of a membrane with no dependence on a concentration gradient. Passive diffusion of a drug that is a weak electrolyte is generally a function of the pKa of the drug and the pH of the compartments across which the drug distributes because only the uncharged form of the drug can diffuse across membranes. When the pKa equals the pH, the amounts of ionized and nonionized forms are equal. The pH values of the major body fluids, which range from 1 to 8, are shown in Table 3. Thus because the drug is ionized slightly in the stomach and appreciably in the blood, it should cross easily from the stomach to the plasma but hardly at all in the reverse direction. This approach is particularly useful for predicting whether drugs can be Distribution to Special Organs and Tissues the rate of blood flow determines the maximum amount of drug that can be delivered per minute to specific organs and tissues at a given plasma concentration. Tissues that are highly perfused, such as the heart, receive a large quantity of drug, provided the drug can cross the membranes or other barriers present.
Super Viagra Dosage and Price
Super Viagra 160mg
- 10 pills - $34.27
- 20 pills - $55.84
- 30 pills - $77.41
- 60 pills - $142.13
- 90 pills - $206.84
- 120 pills - $271.56
- 180 pills - $400.98
Pathology Microscopically best erectile dysfunction doctors nyc discount 160 mg super viagra free shipping, these tumors appear as a pleomorphic or undifferentiated sarcoma, and areas of the liver may be entrapped (see Chapter 89). The cells are spindle or stellate shaped, with without prominent nuclei or well-defined cell borders. Mitotic figures are also present within the tumor, and the cytoplasm and extracellular matrix contain eosinophilic granules (Putra & Ornvold, 2015). Primitive mesenchymal cells with occasional small cysts and ducts lined with benignappearing epithelium are sometimes present at the periphery (Gallivan et al, 1983). Clinical Presentation A right upper quadrant abdominal mass and pain are significant presenting symptoms, and fever also may be prominent. Gastrointestinal symptoms and lethargy may also be present (Putra & Ornvold, 2015). They can be very bulky tumors and sometimes are confused with cystic liver disease (Orozco et al, 1991; Tozzi et al, 1992). These tumors may have the appearance of a solitary liver cyst in childhood (Chowdhary et al, 2004) or may mimic a hydatid cyst (Aggarwal et al, 2001). Treatment and Outcome Embryonal sarcomas of the liver are treated with resection, with or without neoadjuvant chemotherapy, followed by adjuvant chemotherapy (Kadomatsu et al, 1992). Cisplatin, doxorubicin, cyclophosphamide, dacarbazine, actinomycin, vincristine, and other agents have been used in combination with radiotherapy (Newman et al, 1989; Putra & Ornvold, 2015; Vetter et al, 1989). Complete surgical resection should be attempted Future Directions Presently, the need for radiation, or even surgical resection, has been questioned. In the future, some of these patients may be treated by chemotherapy alone after establishment of the diagnosis. If a complete radiologic response is documented after neoadjuvant chemotherapy, no further intervention except observation may be needed, although this requires further study. Embryonal rhabdomyosarcoma of the extrahepatic bile ducts is rare, locally invasive, and requires multidisciplinary treatment. Initial biopsy followed by chemotherapy and resection at a second-look procedure is the standard course. Embryonal Sarcoma Incidence Embryonal sarcoma, also known as malignant mesenchymoma or undifferentiated sarcoma in the older literature, is a rare primary hepatic neoplasm that occurs in older children. The age at diagnosis ranges from 5 to 16 years (Newman et al, 1989; Vetter et al, 1989). Embryonal sarcoma constitutes 14% of malignant liver tumors occurring in children 6 to 10 years of age; however, many of the patients reported recently were older than 10 years (May et al, 2012; Plant et al, 2013; Wei et al, 2008; Yedibela et al, 2000). Malignant Tumors Chapter 95 Hepatic tumors in childhood 1391 and usually requires a major hepatectomy for tumor clearance. Orthotopic transplantation has also shown success when clean margins cannot be obtained with a partial hepatectomy. Although past reports have cited a poor prognosis of 20% to 40% disease-free survival, two recent single-institution series, each with five patients, have reported no recurrence of disease posttreatment, with follow-up ranging from 8 months to 16 years, with a median of 39 months (May et al, 2012; Plant et al, 2013). We have seen long-term survival with a combination of modern multiagent chemotherapy and complete resection. A more recent review identified 34 cases reported between 1970 and 2010, of which only 4 patients were alive at the time of publication (88% mortality). Multivariate analysis was not possible due to the small sample size (Trobaugh-Lotrario et al, 2011). Pathology Histopathologic examination shows a high-grade round-cell neoplasm with abundant cytoplasm and containing cells with cytoplasmic filamentous inclusions (White et al, 1999). The cells are frequently positive for vimentin and cytokeratins, and deletions at chromosome 22q11 are often seen (White et al, 1999). Although leiomyosarcoma may metastasize to the liver from other sites, primary hepatic leiomyosarcoma has been reported in less than 50 patients. It typically arises from the intrahepatic vascular structures, bile ducts, or ligamentum teres. Patients typically present with nonspecific abdominal pain or gastrointestinal symptoms. Biopsy will show intersecting bundles of spindle-shaped cells (Shivathirthan et al, 2011). Adjuvant therapy has not shown significant efficacy; these tumors must be resected for control. Clinical Presentation the diagnosis may be suspected if widespread metastases, including central nervous system dissemination, are found with a hepatic mass. Cases with spontaneous rupture have been reported (Clairotte et al, 2006; Kelly et al, 1998; Ravindra et al, 2002; Yuri et al, 2004). Treatment with dose-intense, antisarcoma-type chemotherapy is also warranted (Trobaugh-Lotrario et al, 2011). Primary Hepatic Rhabdoid Tumor Incidence Rhabdoid tumors are very rare, highly malignant, sarcoma-like neoplasms that usually involve the kidney or central nervous system (Vujanic et al, 1996) (see Chapter 89). They can be primary in extrarenal sites, including extremity, paraspinal, and cervical soft tissues and the liver (Honda et al, 1996; JimenezHeffernan et al, 1998; Kelly et al, 1998). In a literature review of 19 cases of primary hepatic rhabdoid tumor, the median patient age was 16. The overall mortality rate was 89%, and the Outcome Although an initial period of control is feasible, these tumors are likely to recur and metastasize. Angiosarcoma Some authors describe angiosarcoma as the malignant form of hemangioendothelioma in children (Falk et al, 1981; Noronha & Gonzalez-Crussi, 1984) (see Chapter 89). Arsenic exposure has been associated with malignant progression from hemangioendothelioma to hemangiosarcoma (Falk et al, 1981); however, no clear association has been reported between angiosarcoma and arsenic, Thorotrast, or vinyl chloride (Dimashkieh et al, 2004). Histologically, hypercellular whorls of spindled sarcoma cells are observed interspersed with bile ducts, blood vessels, and collagen.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.