
Vasotec
General Information about Vasotec
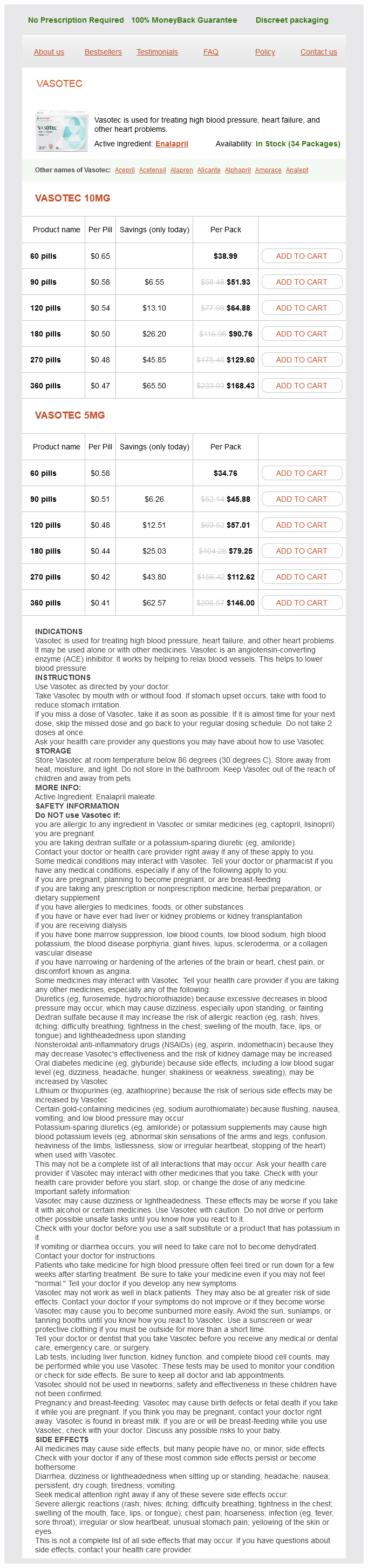
In addition to hypertension, Vasotec can be used for the remedy of coronary heart failure. This is a situation in which the center is unable to pump enough blood to satisfy the body's wants. By relaxing blood vessels, Vasotec reduces the workload on the heart and improves its ability to pump blood successfully. It is commonly prescribed together with different medicines to additional improve heart perform and reduce signs of coronary heart failure.
Vasotec is out there in pill form and is often taken a couple of times a day. The dosage may range relying on the individual's condition and response to the medicine. It is important to comply with the prescribed dosage and to not cease taking Vasotec without consulting a doctor, as sudden discontinuation can result in a dangerous enhance in blood strain.
In conclusion, Vasotec is a useful medication used for the remedy of high blood pressure, heart failure, and other heart issues. By enjoyable blood vessels and bettering blood flow, it helps to lower the danger of great health problems and enhance heart operate. As with any treatment, it may be very important follow the prescribed dosage and converse with a physician if side effects occur. With correct use and monitoring, Vasotec could be an effective software in managing coronary heart well being.
Vasotec may also be used to help stop heart assaults in sufferers with a history of heart disease. It has been proven to scale back the danger of coronary heart attack and death in sufferers who have had a previous coronary heart assault or who've coronary artery disease. This is as a result of Vasotec helps to maintain blood vessels open, permitting blood to move more freely and stopping the formation of blood clots.
High blood pressure, also known as hypertension, is a standard situation during which the drive of blood in opposition to the partitions of the arteries is constantly too high. If left untreated, hypertension can increase the chance of serious health issues, similar to coronary heart attack, stroke, and kidney failure. Vasotec helps to lower blood stress by blocking the motion of angiotensin-converting enzyme (ACE), which is responsible for constricting blood vessels. This allows the blood vessels to loosen up and widen, lowering the strain on the center and enhancing blood flow.
Like any treatment, Vasotec may cause unwanted facet effects in some people. Common unwanted effects embrace dizziness, headache, dry cough, and fatigue. These unwanted effects normally go away as the body adjusts to the medicine. However, if they persist or turn out to be severe, it is essential to speak with a doctor.
Vasotec, also known by its generic name enalapril, is a drugs that belongs to a category of medication called ACE inhibitors. It is often used for treating hypertension, coronary heart failure, and other heart problems. Vasotec works by enjoyable blood vessels, which helps to lower blood strain and enhance blood move, finally resulting in improved coronary heart function.
Vasotec is mostly secure and efficient for most people, however there are certain precautions to maintain in mind. It is not recommended to be used during pregnancy, as it could cause hurt to the creating fetus. It is also necessary to inform the physician of any pre-existing medical situations or medicines being taken, as they could interact with Vasotec and trigger opposed results.
A particular constellation of symptoms referred to as pharyngoconjunctival fever is frequently associated with acute adenovirus infection hypertension table generic vasotec 10 mg fast delivery. In contrast, gastroenteritis has been associated most frequently with serotypes 40 and 41 virus of species F. Immunocompromised patients are highly susceptible to severe disease during infection with respiratory adenoviruses. Papovaviridae: Polyomaviruses Polyomaviruses are small, 1379 Coronaviridae Members of the genus Coronavirus also contribute to respiratory illness, including severe disease. The one major epidemic to date (November 2002 through July 2003) encompassed more than 8000 cases, with mortality rates approaching 10%. Typically, patients present with a nonspecific illness manifesting as fever, myalgia, malaise, and chills or rigors; watery diarrhea may occur as well. Evidence is emerging that this new group 1 coronavirus is a common respiratory pathogen of humans, causing both upper and lower respiratory tract illness. Several cases of respiratory illness have been associated with this virus, but its infrequent identification suggests that this putative group 2 coronavirus has caused a low incidence of illness to date. Studies have shown that humans are infected through direct or indirect contact with infected dromedary camels. Herpesviridae Several herpesviruses cause upper respiratory infections, especially infection of the oral cavity. Herpes simplex pharyngitis is associated with characteristic clinical findings, such as acute ulcerative stomatitis and ulcerative pharyngitis. Primary oral disease can be severe, especially in young children, who sometimes are admitted for rehydration therapy as a result of poor oral intake. A significant proportion of individuals suffer recurrences of symptomatic disease consisting of vesicles on the lips. Parvoviridae: Human Bocavirus A new virus was recently identified in respiratory samples from children with lower respiratory tract disease in Sweden. Sequence analysis of the genome revealed that the virus is highly related to canine minute virus and bovine parvovirus and is a member of the genus Bocavirus (subfamily Parvovirinae, family Parvoviridae). Whether the virus causes or is merely associated with disease remains controversial. Primary infection with most of the acute respiratory viruses often is more severe than secondary infection. Indeed, reinfection with most of these viruses occurs throughout life, but primary infection is much more likely to be associated with severe lower respiratory tract disease, while secondary infection typically is asymptomatic or associated with upper respiratory tract symptoms only. As these infections are ubiquitous, most primary infections (and thus many of the severe cases) occur during the first few years of life. Later, exposure to young children (in populations such as parents of young children and daycare workers) is a risk factor for frequent reinfection. Despite a lifetime of previous exposures, the risk of severe disease increases with age in the elderly, probably because of immune senescence and general medical decline. Typically, there is one dominant virus sweeping through a local community at any one time, a pattern that suggests some population-level interference with transmission. However, outbreaks can be closely spaced, and co-circulation of different viruses or antigenically diverse strains of one virus does occur. Seasons are, of course, reversed in the Northern and Southern hemispheres, so that winter epidemics occur roughly from November to March in the United States but from April to August in Australia; therefore, "winter" epidemics are almost always occurring somewhere in the world. Seasonal variances differ in the tropics, where acute respiratory viral infections are more common in the rainy season. Most single risk factors identified have a moderate effect on the incidence of severe disease, but an accumulation of factors is associated with high risk. Underlying lung disease is a major factor, especially diseases associated with the need for chronic oxygen supplementation. Other severe underlying medical conditions, especially cardiovascular disease, also enhance risk. Smoking (or exposure to wood smoke), low socioeconomic status, and male gender all contribute to a minor increase in the risk of lower respiratory tract illness. A breakdown in isolation and hand-washing compliance procedures can lead to cycles of nosocomial transmission of infection in hospital inpatient wards and intensive care units. In assessments of severe lower respiratory tract illness, a history of travel to an area with unusual agents should be considered carefully. Therefore, contact and droplet precautions are sufficient to prevent transmission in most settings; hand washing is especially critical in health care settings during the winter. Multiplex panels assaying a sample for a dozen or more common respiratory viruses are available. These tests must be used and interpreted carefully because of their extreme sensitivity. In addition, because a viral genome can sometimes persist in nasal secretions for weeks after an infection resolves, a positive test may indicate a recently resolved rather than a currently acute infection. Hypoxia is managed with supplemental oxygen and respiratory failure with mechanical ventilation. Because the tachypnea and fever that often accompany pneumonia and wheezing frequently result in dehydration, fluid management is important. The astute clinician can narrow the etiologic possibilities on the basis of epidemiologic knowledge; information about viruses circulating in the community (widely available from local reference laboratories, county and state health departments, and the U. When diagnostic tests are applied only to samples from individuals at high risk of exposure to an infectious agent in the appropriate season, the positive predictive value of the test is increased.
Even with therapy prehypertension blood pressure values discount vasotec 10 mg fast delivery, neurologic sequelae are common, especially among persons >50 years of age. Occasionally, hypoesthesia and/or weakness of the lower extremities persists for many months. Transitory hypoesthesia of the area of skin innervated by the trigeminal nerve and vestibular system dysfunction (as measured by electronystagmography) are the predominant signs of disease. Whether antiviral chemotherapy can abort these signs or reduce their frequency and severity is not yet known. This uncommon event is usually related to the acquisition of primary infection in the third trimester. Multiple oval ulcerations appear on an erythematous base with or without a patchy white pseudomembrane. Systemic antiviral chemotherapy usually reduces the severity and duration of symptoms and heals esophageal ulcerations. Hematogenous dissemination of virus from sites of oral or genital mucocutaneous disease may also occur, producing bilateral interstitial pneumonitis. Although skin lesions are the most commonly recognized features of disease, many infants do not develop lesions at all or do so only well into the course of disease. Neonatal infection is usually acquired perinatally from contact with infected genital secretions at delivery. The clinical manifestations of recurrent genital herpes-including the frequency of subclinical versus clinical infection, the duration of lesions, pain, and constitutional symptoms-are similar in pregnant and nonpregnant women. First-episode infections in pregnancy have more severe consequences for mother and infant. Maternal visceral dissemination during the third trimester occasionally occurs, as does premature birth or intrauterine growth retardation. Therefore, cesarean section is not warranted for all women with recurrent genital disease. Several studies have shown no correlation between recurrence of viral shedding before delivery and viral shedding at term. Because cesarean section appears to be an effective means of reducing maternalfetal transmission, patients with recurrent genital herpes should be encouraged to come to the hospital early at the time of delivery for careful examination of the external genitalia and cervix as well as collection of a swab sample for viral isolation. The presence of active lesions on the cervix or external genitalia is an indication for cesarean delivery. Point-of-care assays that provide results from capillary blood or serum during a clinic visit are available. However, few available tests report titers, and increases in index values do not reflect first episodes in all patients. A clinical diagnosis can be made accurately when characteristic multiple vesicular lesions on an erythematous base are present. Thus, laboratory studies to confirm the diagnosis and to guide therapy are recommended. For mucocutaneous infections, acyclovir and its congeners famciclovir and valacyclovir have been the mainstays of therapy. Acyclovir, ganciclovir, famciclovir, and valacyclovir are all selectively phosphorylated to the monophosphate form in virus-infected cells. Valacyclovir, the valyl ester of acyclovir, offers greater bioavailability than acyclovir and thus can be administered less frequently. In bone marrow and renal transplant recipients, oral valacyclovir (2 g/d) is also effective in reducing cytomegalovirus infection. First episodes: Oral acyclovir (200 mg 5 times per day or 400 mg tid), valacyclovir (1 g bid), or famciclovir (250 mg bid) for 714 days is effective. Symptomatic recurrent genital herpes: Short-course (1- to 3-day) regimens are preferred because of low cost, likelihood of adherence, and convenience. Oral acyclovir (800 mg tid for 2 days), valacyclovir (500 mg bid for 3 days), or famciclovir (750 or 1000 mg bid for 1 day, a 1500-mg single dose, or 500 mg stat followed by 250 mg q12h for 2 days) effectively shortens lesion duration. Other options include oral acyclovir (200 mg 5 times per day), valacyclovir (500 mg bid), and famciclovir (125 mg bid for 5 days). Suppression of recurrent genital herpes: Oral acyclovir (400800 mg bid) or valacyclovir (500 mg daily) is given. Patients with >9 episodes per year should take oral valacyclovir (1 g daily or 500 mg bid) or famciclovir (250 mg bid or 500 mg bid). First episode: Oral acyclovir is given (200 mg 5 times per day or 400 mg tid); an oral acyclovir suspension can be used (600 mg/m2 qid). Recurrent episodes: If initiated at the onset of the prodrome, single-dose or 1-day therapy effectively reduces pain and speeds healing. Regimens include oral famciclovir (a 1500-mg single dose or 750 mg bid for 1 day) or valacyclovir (a 2-g single dose or 2 g bid for 1 day). Herpetic whitlow: Oral acyclovir (200 mg) is given 5 times daily (alternative: 400 mg tid) for 710 days. Herpetic eye infections: In acute keratitis, topical trifluorothymidine, vidarabine, idoxuridine, acyclovir, penciclovir, and interferon are all beneficial. Continued suppression with oral acyclovir suspension should be given for 34 months. In some patients with milder forms of immunosuppression, oral therapy with valacyclovir or famciclovir is effective.
Vasotec Dosage and Price
Vasotec 10mg
- 60 pills - $38.99
- 90 pills - $51.93
- 120 pills - $64.88
- 180 pills - $90.76
- 270 pills - $129.60
- 360 pills - $168.43
Vasotec 5mg
- 60 pills - $34.76
- 90 pills - $45.88
- 120 pills - $57.01
- 180 pills - $79.25
- 270 pills - $112.62
- 360 pills - $146.00
Thus hypertension nos definition purchase vasotec once a day, Congenital Toxoplasmosis Between 400 and 4000 infants born accurate diagnosis and initiation of appropriate therapy are necessary each year in the United States are affected by congenital toxoplasmosis. Infection of the placenta leads to hematogenous frequency of infection, it has no correlation with the severity of disease infection of the fetus. More than 50% of patients with clinical manifestations have intracerebral involvement. Patients who present with evidence of diffuse cortical dysfunction develop evidence of focal neurologic disease as infection progresses. This altered condition is due not only to the necrotizing encephalitis caused by direct invasion by the parasite but also to secondary effects, including vasculitis, edema, and hemorrhage. The onset of infection can range from an insidious process over several weeks to an acute presentation with fulminant focal deficits, including hemiparesis, hemiplegia, visual-field defects, localized headache, and focal seizures. Brainstem involvement gives rise to a variety of neurologic dysfunctions, including cranial nerve palsy, dysmetria, and ataxia. With basal ganglion infection, patients may develop hydrocephalus, choreiform movements, and choreoathetosis. Involvement of the pituitary gland can give rise to panhypopituitarism and hyponatremia from inappropriate secretion of vasopressin (antidiuretic hormone). Autopsies of Toxoplasma-infected patients have demonstrated the involvement of multiple organs, including the lungs, gastrointestinal tract, pancreas, skin, eyes, heart, and liver. Respiratory involvement usually presents as dyspnea, fever, and a nonproductive cough and may rapidly progress to acute respiratory failure with hemoptysis, metabolic acidosis, hypotension, and (occasionally) disseminated intravascular coagulation. The presence of organisms is a helpful diagnostic indicator, but organisms can also be found in healthy tissue. Infection of the heart is usually asymptomatic but can be associated with cardiac tamponade or biventricular failure. Factors associated with relatively severe disabilities include delays in diagnosis and in initiation of therapy, neonatal hypoxia and hypoglycemia, profound visual impairment (see "Ocular Infection," below), uncorrected hydrocephalus, and increased intracranial pressure. If treated appropriately, upwards of 70% of children have normal developmental, neurologic, and ophthalmologic findings at follow-up evaluations. Treatment for 1 year with pyrimethamine, a sulfonamide, and folinic acid is tolerated with minimal toxicity (see "Treatment," below). It was formerly thought that the majority of cases of ocular disease were due to congenital infection. New ocular toxoplasmosis in immunocompetent individuals occurs more commonly than was previously appreciated and has been associated with outbreaks in Victoria (British Columbia) and in South America. A variety of ocular manifestations are documented, including blurred vision, scotoma, photophobia, and eye pain. Macular involvement occurs, with loss of central vision, and nystagmus is secondary to poor fixation. Involvement of the extraocular muscles may lead to disorders of convergence and to strabismus. Ophthalmologic examination should be undertaken in newborns with suspected congenital infection. As the inflammation resolves, vision improves, but episodic flare-ups of chorioretinitis, which progressively destroy retinal tissue and lead to glaucoma, are common. The ophthalmologic examination reveals yellow-white, cotton-like patches with indistinct margins of hyperemia. As the lesions age, white plaques with distinct borders and black spots within the retinal pigment become more apparent. Lesions usually are located near the posterior pole of the retina; they may be single but are more commonly multiple. Congenital lesions may be unilateral or bilateral and show evidence of massive chorioretinal degeneration with extensive fibrosis. Histologic examination of lymph nodes may suggest the characteristic changes described above. Demonstration of tachyzoites in lymph nodes establishes the diagnosis of acute toxoplasmosis. Like subinoculation into mice, histologic demonstration of cysts containing bradyzoites confirms prior infection with T. Positive IgG titers (>1:10) can be detected as early as 23 weeks after infection. These titers usually peak at 68 weeks and decline slowly to a new baseline level that persists for life. Antibody avidity increases with time and can be useful in difficult cases during pregnancy for establishing when infection may have occurred. Both assays are specific and sensitive, with fewer false-positive results than other commercial tests. Although a negative IgM result with a positive IgG titer indicates distant infection, IgM can persist for >1 year and should not necessarily be considered a reflection of acute disease. If acute toxoplasmosis is suspected, a more extensive panel of serologic tests can be performed. Molecular Diagnostics Molecular approaches can directly Serology Because some diagnostic tests are available only at spe- detect T. Isolates can be genotyped and polymorphic sequences can be obtained, with consequent identification of the precise strain.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.