
Viagra Professional
General Information about Viagra Professional
Another advantage of Viagra Professional is its longer period of action. While regular Viagra can last up to 4 hours, the effects of Viagra Professional can last up to six hours. This makes it a more handy option for those seeking to interact in sexual exercise a number of occasions within a brief interval.
Like regular Viagra, Viagra Professional works by increasing blood flow to the penis, which helps in reaching and sustaining an erection throughout sexual stimulation. However, the higher focus of sildenafil citrate in Viagra Professional permits for a stronger and longer-lasting erection, giving men the confidence and talent to perform higher within the bed room.
Viagra Professional is on the market within the form of oral tablets and must be taken as prescribed by a well being care provider. It should not be taken greater than as quickly as a day and shouldn't be used with certain medications or medical circumstances. It is crucial to inform a health care provider about any pre-existing medical conditions or medicines being taken before beginning therapy with Viagra Professional.
As an extra-strength model of Viagra, Viagra Professional is designed to provide faster and longer-lasting results. One of the key variations between common Viagra and Viagra Professional is the focus of the energetic ingredient, sildenafil citrate. While common Viagra accommodates 50mg or 100mg of sildenafil citrate, Viagra Professional incorporates 100mg, making it stronger and effective.
One of the principle advantages of Viagra Professional is its quicker onset of motion. While common Viagra could take as a lot as an hour to begin out working, Viagra Professional can start working in as little as 20 minutes. This is as a outcome of the higher focus of sildenafil citrate in Viagra Professional increases the rate at which the drug is absorbed into the bloodstream.
Viagra Professional is a extremely efficient prescription medicine that has helped hundreds of thousands of men around the globe with erectile dysfunction (ED). Also often identified as sildenafil citrate, this drug is a well-known and broadly used treatment for ED. However, Viagra Professional takes the effectiveness of the long-lasting blue capsule to the following level.
It is important to note that like any medicine, Viagra Professional could trigger unwanted aspect effects. These unwanted effects are usually mild and momentary, and should embody headache, dizziness, facial flushing, or upset abdomen. However, if symptoms persist or become severe, it's important to consult a healthcare skilled.
Moreover, the extra-strength method of Viagra Professional is designed to offer a extra consistent and dependable response. This means that males taking Viagra Professional can experience improved sexual efficiency and satisfaction with each use.
In conclusion, Viagra Professional is an extra-strength version of the well-known ED medication, Viagra. With the next concentration of the active ingredient, sildenafil citrate, it offers faster onset of action, longer duration of results, and a more constant response. It is a extremely effective option for men in search of a stronger and dependable therapy for ED. However, it's essential to consult a physician and observe the prescribed dosage and utilization directions to make sure safe and efficient results.
This type of alopecia can occur about 2 to 4 months after a severe disease flare and cause massive hair shedding impotence divorce buy cheap viagra professional. This hair loss is permanent because the hair follicles are damaged by the inflammation. May impair hydroxychloroquine effect · Hydroxychloroquine: may take 3 months to see the effect. Identify manifestations of lupus that warrant high-dose (prednisone 1 mg/kg/day) corticosteroid therapy. Although septic arthritis is always a concern, this presentation is worrisome for osteonecrosis of the hip (see Chapter 54: Osteonecrosis). Patients on immunosuppressive agents and/or prednisone 20 mg/day may not mount a satisfactory immune response. What is the utility of following serologic tests to assess disease activity and predict disease flares Data supports that individual patients act differently but usually fall into one of three patterns: 1. Always serologically active and may never flare Therefore, the clinician needs to establish the serologic pattern for each patient and treat accordingly. Only patients who demonstrate that they flare when their serologies become more active should receive prophylactic increases in immunosuppression to prevent a flare. The disease activity measures give an assessment of the degree of active inflammation, whereas the damage scores give an idea of the downstream effects of the disease or therapies. Autologous bone marrow transplant using various conditioning regimens has been completed in a small number of patients. Other studies report a high incidence of treatment-related complications such as infection. The overall 5-year survival rate has improved in the last 20 years to 95% and 10-year survival to 90% likely due to earlier diagnosis and aggressive management of comorbidities. However, mortality is increased three times Downloaded for Anonymous User (n/a) at Egyptian Knowledge Bank from ClinicalKey. Death early in the disease is generally a reflection of active lupus or its treatment (infection), whereas death late in disease is due to active disease, atherosclerosis, and malignancy. The most common causes of death are: · Infection: accounts for 20% to 25% of all deaths and increased five times compared with the general population. All infections (bacterial, fungal, tuberculous, nontuberculous mycobacterial, viral) are increased mostly related to the complications of immunosuppressive therapy, especially due to prolonged use of high-dose corticosteroids. For each increase of prednisone by 10 mg/day, the risk of serious infection increases 11-fold. Hematopoetic and mesenchymal stem cell transplantation in the treatment of refractory systemic lupus erythematosus-where are we now A longitudinal analysis of outcomes of Lupus nephritis in an international inception cohort using a multistate model approach. Derivation and validation of the systemic lupus international collaborating clinics classification criteria for systemic lupus erythematosus. The effect of moderate-dose corticosteroids in preventing severe flares in patients with serologically active, but clinically stable, systemic lupus erythematosus: findings of a prospective, randomized, double-blind, placebo-controlled trial. The classification of glomerulonephritis in systemic lupus erythematosus revisited. Overall and cause specific mortality in patients with systemic lupus erythematosus: a metaanalysis of observational studies. The development of drug-induced autoantibodies is much more common than the development of lupus-like disease. Usually with photosensitivity and can be associated with other cutaneous lesions. It usually occurs 1 to 5 months after initiating therapy with the offending medication. How do the clinical manifestations of procainamide-induced lupus differ from those of hydralazine-induced lupus Patients with procainamide-induced disease are more likely to have pleuritis and/or pericarditis, whereas patients with hydralazine-induced disease are more likely to have rashes. Most patients (95%) with symptomatic drug-induced disease due to procainamide, hydralazine, chlorpromazine, and quinidine demonstrate elevated levels of IgG antihistone antibodies. As discussed, nearly all patients (95%) with symptomatic procainamide- or hydralazine-induced lupus demonstrate elevated serum levels of IgG antihistone antibodies. Furthermore, some patients taking either procainamide or hydralazine will have a positive test but not have symptoms of a lupus-like disease. In certain specialized research laboratories, the specificity of antihistone antibodies for individual histones. Overall, antihistone Downloaded for Anonymous User (n/a) at Egyptian Knowledge Bank from ClinicalKey. Fever (38%), rash (20% to 30%), pleuritis/pneumonitis (10%), hepatitis (50% with elevated liver-associated enzymes), and anticardiolipin antibodies (33%) can be seen. It is usually triggered by fluorouracil compounds or their modern derivatives such as capecitabine. The major risk for procainamideor hydralazine-induced lupus appears to be acetylator phenotype. Metabolism of these drugs involves the hepatic Downloaded for Anonymous User (n/a) at Egyptian Knowledge Bank from ClinicalKey. Nonsteroidal antiinflammatory drugs will often help control the symptoms such as arthralgias, as the disease gradually resolves after the drug is stopped. Patients with more severe signs and symptoms, especially those with pericarditis or pleuritis, often require a short course of corticosteroids to control their disease. Editorial: the innate and adaptive immune response are both involved in drug-induced autoimmunity.
Patients with metabolic myopathies typically present with one of the following: · Metabolic myopathies presenting with exercise intolerance erectile dysfunction treatment boots viagra professional 50 mg otc, severe prolonged cramps, and red-wine or colacolored urine (indicating myoglobinuria). If symptoms (usually myalgias and myoglobinuria without cramps) occur only after prolonged exercise and are worse during fasting, then lipid storage disease. Once a detailed history and physical examination are performed, measurement of muscle enzymes and electrodiagnostic studies follow if complaints are suspicious for myopathy. Levels are generally normal, except for patients with McArdle disease (myophosphorylase deficiency). A positive result can be confirmed by genetic testing or muscle biopsy enzyme analysis. A muscle biopsy can provide important diagnostic information in the evaluation of a patient with a metabolic muscle disease. Magnetic resonance spectroscopy is another tool useful for the in vivo evaluation of muscle energetics. Magnetic resonance imaging has been used to identify sites of abnormal tissue and as a guide for muscle biopsy. Many metabolic myopathy specialists have moved to a genetic testing first approach. This inverted diagnostic stratagem still may require clinicians to circle back around to ancillary testing to help clarify variants of undetermined significance found on next generation sequencing panels, exomes, or genomes. This test exploits the abnormal biochemistry that results in the absence of those enzymes. Normal muscle generates lactate from the degradation of glycogen when it exercises. With defects in glycolysis or glycogenolysis, pyruvate is not produced under anaerobic conditions, and thus no lactate can be generated by lactate dehydrogenase. In addition, ammonia, inosine, and hypoxanthine concentrations increase significantly. A blood sample for analysis of baseline lactate, ammonia, and pyruvate levels is drawn through an indwelling catheter in an antecubital vein (preferably placed without use of a tourniquet) 2. In the past, a sphygmomanometer cuff was placed on the upper arm of the side with the indwelling catheter and inflated to at least 20 mmHg above systolic pressure. However, the blood pressure cuff is not necessary and can lead to forearm rhabdomyolysis and compartment syndrome, especially in patients with McArdle disease. The subject rhythmically squeezes a tennis ball or similar object at maximal intensity for 14 seconds followed by a 1-second reprieve for a total of 60 seconds. After the 60 seconds of exercise, additional venous samples for lactate and ammonia are obtained at 1, 2, 4, 6, and 10 minutes thereafter. As they are drawn, the blood vials should be placed on ice and immediately transported to the laboratory and processed. In normal individuals, lactate and ammonia increase at least two and half times baseline values in the first two samples after exercise and then gradually decrease toward baseline. The major reason for a false-positive result is insufficient work by the individual while exercising. If lactate (and pyruvate) does not rise but ammonia does, the patient may have a defect in glycolysis, such as McArdle disease. Why is muscle biopsy a valuable diagnostic tool in the evaluation of metabolic myopathies Muscle biopsy for routine histologic, histochemical, and ultrastructural analysis (electron microscopy) is helpful in evaluating a suspected metabolic myopathy, primarily because it helps rule out other conditions that can cause muscle dysfunction and allows testing for deficiencies or absence of specific glycolytic pathway enzymes. The most important studies are listed below: Stain Periodic acid-Schiff Sudan black or Oil red O Gomori Acid phosphatase Specific enzymes: 20. What is the approach to evaluation and management of a patient with rhabdomyolysis and myoglobinuria After a single episode of exertional rhabdomyolysis, the risk of recurrence is quite low, and further evaluation may not be warranted. For patients with multiple, recurrent episodes of rhabdomyolysis, the most reasonable first step now, with the availability of large genetic testing panels at relatively low cost, is to order genetic testing covering 30500 muscle genes (inclusive of the metabolic myopathy genes). Describe common genetic muscle diseases that may be confused with metabolic myopathies and childhood or adult polymyositis. Calf hypertrophy, scoliosis, loss of ambulation by age 13, and death from respiratory failure or cardiomyopathy in the third and fourth decades occurred in the past. Diagnosis is by genetic testing, and genetic therapies are now available to significantly slow the progression of disease. Becker dystrophy: X-linked disease due to a less severe mutation of the dystrophin gene resulting in a partially functional protein complex. Similar to Duchenne dystrophy, but milder, with patients able to walk beyond the age of 16 years. The extent of skeletal muscle and cardiac muscle dysfunction may be quite discordant with some ambulatory Becker patients requiring cardiac transplantation. An equal percentage may manifest cardiac dysfunction, arrhythmias, or heart failure, clinically or on testing (heart monitors and echocardiograms). Whenever a woman with muscle disease has symptoms that do not fit into a typical diagnosis, genetic muscle disease can be considered. Variable disease expression with disease onset between adolescence and middle-adult years. Fortunately, with large genetic testing panels encompassing 80 to 500 genes, many of these genetic muscles disease can be cost-effectively diagnosed early in the evaluation. Patients present with progressive lower extremity followed by upper extremity proximal muscle weakness beginning in second to fourth decades. The disease slowly progresses leading to 50% of patients requiring wheelchair use in 1030 years. A diagnostic clue is that most patients have difficulty standing on their toes within the first 12 years of symptom onset due to early, concomitant calf muscle weakness.
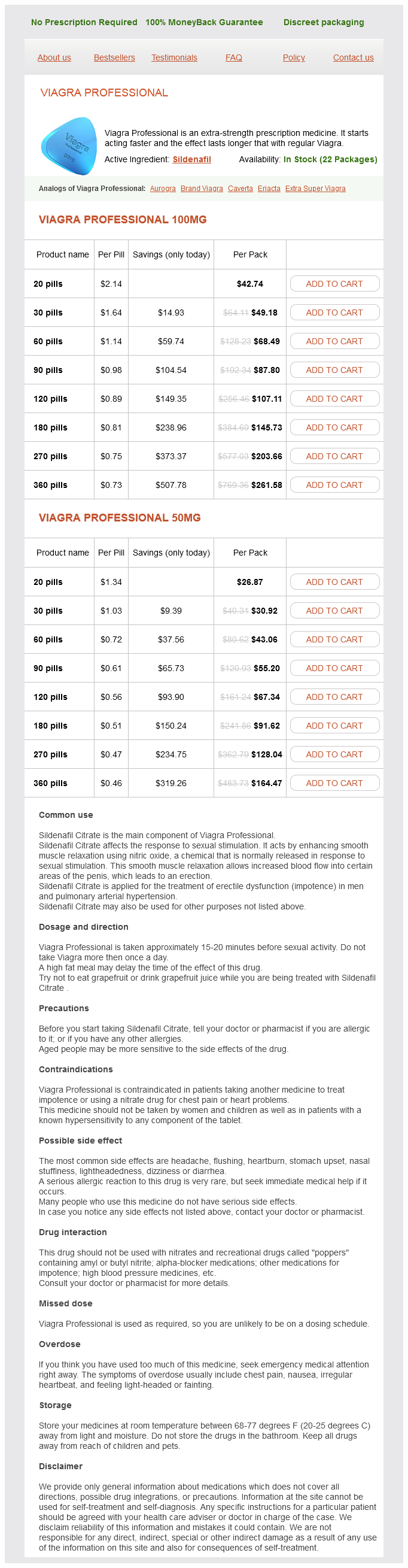
Viagra Professional Dosage and Price
Viagra Professional 100mg
- 20 pills - $42.74
- 30 pills - $49.18
- 60 pills - $68.49
- 90 pills - $87.80
- 120 pills - $107.11
- 180 pills - $145.73
- 270 pills - $203.66
- 360 pills - $261.58
Viagra Professional 50mg
- 20 pills - $26.87
- 30 pills - $30.92
- 60 pills - $43.06
- 90 pills - $55.20
- 120 pills - $67.34
- 180 pills - $91.62
- 270 pills - $128.04
- 360 pills - $164.47
Transcriptional profiling of stroma from inflamed and resting lymph nodes defines immunological hallmarks erectile dysfunction freedom viagra professional 50 mg online. Stromal and hematopoietic cells in secondary lymphoid organs: partners in immunity. Regulatory T cells expressing interleukin 10 develop from Foxp3 1 and Foxp3 2 precursor cells in the absence of interleukin 10. Clonal deletion of thymocytes can occur in the cortex with no involvement of the medulla. Aire controls gene expression in the thymic epithelium with ordered stochasticity. An interaction between kynurenine and the aryl hydrocarbon receptor can generate regulatory T cells. Clonal expansion versus functional clonal inactivation: a costimulatory signalling pathway determines the outcome of T cell antigen receptor occupancy. Deletional self-tolerance to a melanocyte/melanoma antigen derived from tyrosinase is mediated by a radio-resistant cell in peripheral and mesenteric lymph nodes. Recent thymic emigrants are the preferential precursors of regulatory T cells differentiated in the periphery. Overlapping gene coexpression patterns in human medullary thymic epithelial cells generate self-antigen diversity. Breakdown of a single mechanism of self-tolerance causes various autoimmune diseases. Population and single-cell genomics reveal the Aire dependency, relief from Polycomb silencing, and distribution of self-antigen expression in thymic epithelia. A wave of regulatory T cells into neonatal skin mediates tolerance to commensal microbes. Commensal microbes and hair follicle morphogenesis coordinately drive Treg migration into neonatal skin. Positive and negative selection of an antigen receptor on T cells in transgenic mice. How specificity for self-peptides shapes the development and function of regulatory T cells. Pancreatic gene expression in rare cells of thymic medulla: evidence for functional contribution to T cell tolerance. Transcription of a broad range of selfantigens in human thymus suggests a role for central mechanisms in tolerance toward peripheral antigens. Murine thymic selection quantified using a unique method to capture deleted T cells. Autoreactive T and B cells responding to myelin proteolipid protein in multiple sclerosis and controls. Pancreatic -cells limit autoimmune diabetes via an immunoregulatory antimicrobial peptide expressed under the influence of the gut microbiota. T-cell apoptosis detected in situ during positive and negative selection in the thymus. Fezf2 orchestrates a thymic program of self-antigen expression for immune tolerance. Detection of an autoreactive T-cell population within the polyclonal repertoire that undergoes distinct autoimmune regulator (Aire)-mediated selection. Immunization of guinea pigs against lymphocytic choriomeningitis with formolized tissue vaccines. Murine autoimmune oophoritis, epididymoorchitis, and gastritis induced by day 3 thymectomy. Epigenetic regulation of promiscuous gene expression in thymic medullary epithelial cells. Ectopic expression of peripheral-tissue antigens in the thymic epithelium: probabilistic, monoallelic, misinitiated. Regulatory T-cell differentiation versus clonal deletion of autoreactive thymocytes. Requirement for cotolerogenic gene products in the clonal deletion of I-E reactive T cells. Thymic B cells are licensed to present self antigens for central T cell tolerance induction. Regulatory T cells generated early in life play a distinct role in maintaining self-tolerance. Identification of a previously unknown antigen-specific regulatory T cell and its mechanism of suppression. Thymus-homing peripheral dendritic cells constitute two of the three major subsets of dendritic cells in the steady-state thymus. While the innate immune system utilizes a relatively small number of invariant receptors specific for conserved microbial products, such as the cell wall components of bacteria, the adaptive immune system makes use of a nearly unlimited repertoire of receptors generated by random recombination of the T- and B-cell receptor loci. Although random recombination allows for incredible lymphocyte receptor diversity, it comes at the price of generating potentially autoreactive receptors. The risk for self-reactivity is in part mitigated by checkpoints during lymphocyte development that eliminate most of the self-reactive clones (referred to as central tolerance) as well as mechanisms that limit the ability of self-reactive clones to mount responses in the periphery (referred to as peripheral tolerance). However, the existence of lymphocyte-dependent autoimmune disease is a clear indication that these mechanisms are imperfect and some self-reactive lymphocytes are able to initiate destructive autoimmune inflammation.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.