
Vimax
General Information about Vimax
Vimax additionally accommodates Saw Palmetto, a herb that has been used for its aphrodisiac properties. This ingredient helps to spice up libido and sexual desire, making it a superb addition to the formula. By growing sexual stamina, it permits men to last more in bed and fulfill their partner�s wants.
Apart from bettering sexual performance, Vimax additionally helps to enhance overall sexual well being. It works by nourishing the reproductive system and selling the manufacturing of testosterone, the male intercourse hormone answerable for libido, sperm production, and muscle mass. This makes it a superb supplement for males who want to preserve their sexual well being and virility as they age.
Another important ingredient in Vimax is Ginkgo Biloba, a strong antioxidant that helps to improve blood circulate and circulation. This helps to increase the oxygen and nutrient provide to the penis, selling wholesome tissue progress and bettering overall sexual function. It additionally helps to reduce back anxiousness and stress, which are frequent barriers to reaching and sustaining an erection.
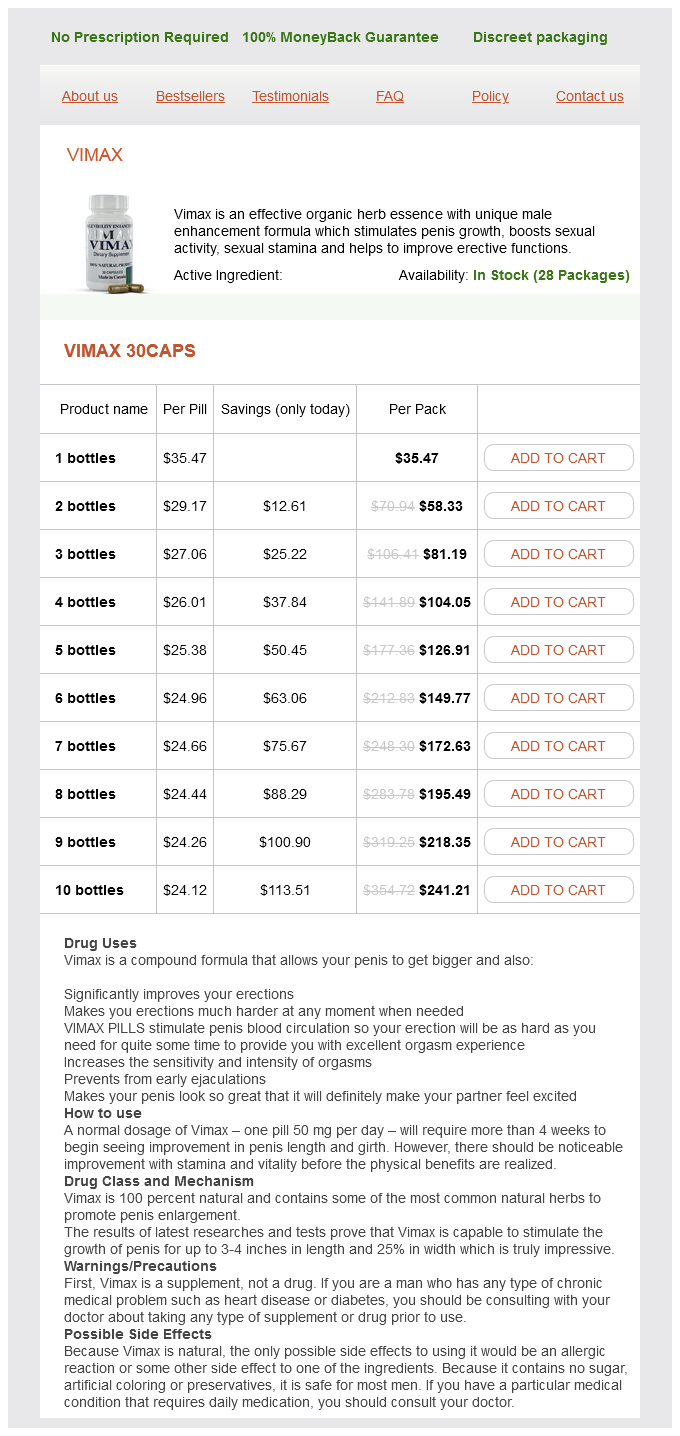
In conclusion, Vimax is an efficient organic herb essence with a singular male enhancement formula that has proven to be a game-changer for males fighting sexual performance points. Its highly effective mix of natural elements not only stimulates penis progress and boosts sexual exercise, however it also improves sexual stamina and erectile perform. So, if you would like to take charge of your sexual well being and expertise a satisfying and fulfilling sex life, Vimax is definitely price contemplating.
In addition to its formulation, what makes Vimax stand out is its ease of use. It comes within the form of a tablet, making it easy to include into your daily routine. You can discreetly take it with a glass of water, and there�s no want for any particular devices or tools. This makes it a handy and hassle-free option for men who wish to experience its advantages with none complications.
Vimax is a premium organic herb essence that has taken the male enhancement market by storm. It has gained a status as a extremely effective and safe way to address issues related to sexual efficiency and satisfaction. Made from natural ingredients and backed by scientific analysis, this complement has turn into the go-to resolution for men trying to improve their sexual well being.
One of the vital thing elements in Vimax is Horny Goat Weed, a herb that has been used for centuries in conventional Chinese medication. It works by growing the production of nitric oxide within the physique which helps to chill out blood vessels and improve blood flow to the penis. This results in stronger and longer-lasting erections, making it a highly effective treatment for erectile dysfunction.
One of probably the most important benefits of Vimax is its natural nature. Unlike different male enhancement products which are filled with chemical substances and artificial components, Vimax is made from 100 percent pure elements. This signifies that it's safe to use and has little to no unwanted aspect effects. It can additionally be free from harmful substances like steroids, synthetic colours, and flavors, making it a more healthy and more appealing choice for men.
What units Vimax apart from different male enhancement products is its unique method that stimulates penis progress and boosts sexual activity. This powerful mixture of natural elements works collectively to deliver a complete answer for males of all ages. Whether you're dealing with points related to erectile dysfunction, low libido, or a small penis dimension, Vimax has received you covered.
Number of lymph node metastases is a significant prognostic factor in intrahepatic cholangiocarcinoma erectile dysfunction natural shake buy cheap vimax 30 caps online. Indications for surgical treatment of intrahepatic cholangiocarcinoma with lymph node metastases. Liver resection for hilar and peripheral cholangiocarcinomas: a study of 62 cases. Effects of 5-fluorouracil and leucovorin in the treatment of pancreaticbiliary tract adenocarcinomas. Effective treatment of advanced biliary tract carcinoma using 5-fluorouracil continuous infusion with cisplatin. Comparison of 5-fluorouracil, doxorubicin and mitomycin C with 5-fluorouracil alone in the treatment of pancreaticbiliary carcinomas. Treatment of advanced adenocarcinomas of the exocrine pancreas and the gallbladder with 5-fluorouracil, high dose levofolinic acid and oral hydroxyurea on a weekly schedule. Outpatient therapy with gemcitabine and docetaxel for gallbladder, biliary, and cholangiocarcinomas. Gemcitabine and irinotecan in locally advanced or metastatic biliary cancer: preliminary report. Gemcitabine concurrent with continuous infusional 5-fluorouracil in advanced biliary cancers: a review of the Princess Margaret Hospital experience. A multicenter retrospective analysis of survival benefits of chemotherapy for unresectable biliary tract cancer. Unexpected response to systemic chemotherapy in case of primarily nonresectable advanced disseminated intrahepatic cholangiocarcinoma. Transcatheter arterial chemoembolization or chemoinfusion for unresectable intrahepatic cholangiocarcinoma: clinical efficacy and factors influencing outcomes. Transarterial chemoembolization is a safe treatment for unresectable hepatic malignancies. Initial experience from a combination of systemic and regional chemotherapy in the treatment of patients with nonresectable cholangiocellular carcinoma in the liver. Hepatic intraarterial chemotherapy with gemcitabine in patients with unresectable cholangiocarcinomas and liver metastases of pancreatic cancer: a clinical study on maximum tolerable dose and treatment efficacy. Transcatheter arterial chemoembolization in unresectable cholangiocarcinoma: initial experience in a single institution. Radiation therapy is associated with improved survival in the adjuvant and definitive treatment of intrahepatic cholangiocarcinoma. Treatment of unresectable hepatocellular carcinoma with use of 90Y microspheres (TheraSphere): safety, tumor response, and survival. Radioembolization with Yttrium-90 microspheres: review of an emerging treatment for liver tumors. Radiation lobectomy: preliminary findings of hepatic volumetric response to lobar yttrium-90 radioembolization. Treatment of unresectable cholangiocarcinoma using yttrium-90 microspheres: results from a pilot study. Yttrium-90 radiotherapy for unresectable intrahepatic cholangiocarcinoma: a preliminary assessment of this novel treatment option. Retrospective analysis of prognostic factors after liver resection and transplantation for cholangiocellular carcinoma. Liver transplantation for cholangiocellular carcinoma: analysis of a single-center experience and review of the literature. Liver transplantation as a primary indication for intrahepatic cholangiocarcinoma: a single-center experience. Radiologic spectrum of cholangiocarcinoma: emphasis on unusual manifestations and differential diagnoses. Limitations of the histopathological diagnosis and prognostic assessment of hepatocellular carcinoma. Clinicopathological features and outcome of hepatic resection for intrahepatic cholangiocarcinoma in Japan. Clinical characteristics and proliferating activity of intrahepatic cholangiocarcinoma. Analysis of the relationships between clinicopathologic factors and survival time in intrahepatic cholangiocarcinoma. Arterial chemoinfusion therapy through an implanted port system for patients with unresectable intrahepatic cholangiocarcinoma- initial experience. In Delhi in north India, it is the fourth most common cancer (following breast 30, cervix 22, and ovary 10) and the most common gastrointestinal cancer in women. It is rare in the United States, United Kingdom, Western Europe, Australia, and New Zealand with incidence rates in women approximately 1. Bacterial Infection It has been postulated that bacterial infection associated with gallstones might result in the formation, in bile, of local high concentrations of carcinogens. More recently, reporting on 44 patients with porcelain gallbladder, Stephen et al. The possibility of a polyp being malignant increases with the age of the patient, increasing size of the lesion, when the lesion is sessile rather than pedunculated, single rather than multiple, and is associated with gallstones. There are reports of a positive association with total calorie intake, high carbohydrate intake, and an inverse association with dietary fiber intake and micronutrients in vegetables and fruits, vitamin C and vitamin E. A special mention should be made of jaundice as it is an ominous sign that portends advanced disease, most unlikely to be cured by surgical intervention. Patients with metastatic disease may have a nodular liver, ascites, umbilical nodule, and enlarged left supraclavicular lymph nodes. Cross-sectional imaging usually reveals one of the following patterns: (1) focal or diffuse mural thickening, (2) intraluminal polypoidal mass originating from gallbladder wall, and (3) a subhepatic mass replacing or obscuring the gallbladder and often infiltrating the adjacent liver. Polypoidal lesions enhance homogenously whereas infiltrative lesions show irregular enhancement with areas of necrosis.
Neurologic workup is not necessary with every new patient erectile dysfunction rap buy vimax 30 caps low price, but if the headache is atypical or has recently changed or there is a history of red flags, a search for underlying disease is warranted (Table 1. In formulating the differential diagnoses of the primary headaches, it is useful to follow a sequence of steps (Table 1. First, classify the headaches in to low or high frequency (less or more than 15 headache days per month). Finally, consider headaches of short duration of low or high frequency and the presence or not of triggering factors. Late life migraine accompaniments as a cause of unexplained transient ischemic attacks. Shortlasting unilateral neuralgiform headache attacks with conjunctival injection, tearing, sweating, and rhinorrhea. Although the vast majority of headache syndromes are benign, clinicians are faced with the crucial task of differentiating benign headache disorders from potentially life-threatening conditions. Given the broad range of disorders that present with headache, a focused and systematic approach is necessary to facilitate the prompt diagnosis and treatment of various kinds of head pain. In managing a patient with chronic, recurrent primary headaches, there must be a positive interrelationship between patient and doctor. During the initial evaluation, the patient and the doctor should get to know one another. If worrisome features or "red flags" are present either in the history or on examination, diagnostic testing may be necessary to exclude secondary headache disorders. Having determined that the condition is a primary headache, the specific headache type must be diagnosed. Once a diagnosis has been established, the general therapeutic options should be outlined in a treatment plan tailored to the patient. One should emphasize the need for the patient to be active in his or her own care. Realistic expectations should be established, and rarely will the initial plan be perfect. Follow-up visits are scheduled to modify the therapy and, if necessary, to reassess the diagnosis. History-taking is often complicated by the presence of more than one type of headache or by a change in the headache pattern over time. It is often helpful to begin with the current headache of greatest concern to the patient and subsequently explore other headache patterns and the evolution of those patterns. The doctor will have a general idea about the degree of disability after speaking to the patient. More specifically, we want to know how the headaches are impacting on family life, schoolwork or occupation, and social life. Age at onset and at presentation Most of the primary headache disorders begin in childhood or early adult life. Like migraine, tension-type headache and cluster headache may start in early childhood or later in life, but commonly occur between the ages of 20 and 30 years. Without an adequate history, unnecessary diagnostic and treatment interventions may be performed or, alternatively, crucial testing may not be obtained. Taking the headache history provides an opportunity to establish a rapport with the patient that will serve as the basis for an ongoing therapeutic relationship. Headache descriptors should first be sought with open-ended statements such as "Tell me about your headaches and how they impact your life. With advancing age, headache or facial pain may result from medications, systemic disorders, postherpetic neuralgia, trigeminal neuralgia, or disorders of the head, neck, eyes, ears, or nose. For these reasons, testing is indicated when older patients present with headaches of recent onset, headaches that have changed from a pre-existing pattern, or headaches that are associated with an abnormal examination. The location of headache in a patient with migraine may fluctuate over the course of an attack and between different attacks. However, the latter two headache types may last for days or may evolve in to a chronic form. The timing of headaches within a diurnal, monthly, or annual cycle is particularly important in the diagnosis of cluster headache. Changes in the frequency of headache may be the cause of the visit to the physician, as when relatively well-controlled attacks of migraine increase in frequency or transform in to a daily or near-daily headache. Frequent episodic and chronic headaches are managed differently from a rarely occurring headache. The frequency and timing of headache attacks within a longer period of time, such as months or a year or more, allow an understanding of the burden of headache for the individual. Infratentorial, occipitonuchal, and cervical spine pathology can refer pain to the forehead or eye because of the convergence of cervical nociceptive afferents at the second and third cervical levels with trigeminal afferents in the caudal trigeminal nucleus of the brainstem. As blood or pus tracks down the subarachnoid space, the acute headache of a subarachnoid hemorrhage or meningitis may be followed by pain that travels down the spinal column to the interscapular region or lower back. Burning or pulsating ocular or periorbital pain may reflect incipient ischemia in the vertebrobasilar territory, an expanding skull base aneurysm, extracranial or intracranial vascular dissection, dural sinus occlusion, or inflammation in the cavernous sinus. Ask the patient to grade the intensity on a scale of 1 to 10, with 1 as pain that can barely be appreciated and 10 as the worst pain possible. The intensity of a tension-type headache is rarely more than moderate, migraine is usually moderate to severe, and cluster headaches are unbearably severe.
Vimax Dosage and Price
Vimax 30caps
- 1 bottles - $35.47
- 2 bottles - $58.33
- 3 bottles - $81.19
- 4 bottles - $104.05
- 5 bottles - $126.91
- 6 bottles - $149.77
- 7 bottles - $172.63
- 8 bottles - $195.49
- 9 bottles - $218.35
- 10 bottles - $241.21
During gas molecule collisions erectile dysfunction protocol foods effective 30 caps vimax, kinetic energy is temporarily converted in to potential energy. As the average intermolecular distance increases with increasing volume of a gas, there is a drop in the number of collisions that occur per unit time, which results in an overall decrease in average potential energy of the gas. Since total energy of the gas is conserved during isenthalpic expansion, this leads to an increase in kinetic energy and thus temperature of the gas. Above the inversion temperature, the latter effect dominates, and isenthalpic free expansion of the gas causes a temperature increase. The technique itself uses a cycle of subsequent freezing, thawing, and re-freezing tissue to induce osmotic shifts that result in cellular membrane rupture and eventual cell death within target tissue. The cell killing effects of cryoablation may be the result of any of a number of proposed pathways. Proposed mechanisms include direct cytolysis via intracellular and extracellular ice crystal formation causing protein denaturation, intracellular dehydration and pH changes, ischemic necrosis via vascular injury, cellular edema and vessel disruption incurred during the thaw phase, or activation of antitumor immune responses and induction of cellular apoptosis. In addition, endothelial damage resulting from cryoablation leads to platelet aggregation and microthrombosis. Frozen tissue is visualized as a well-defined, expanding "ice-ball" that is lower in density than normal surrounding tissue. Although ultrasound can also depict the effects of freezing in real time, complete visualization of the ablation zone is limited due to echogenic shadowing from the proximal edge of the ice-ball as it forms during treatment. The number of freeze-thaw-freeze cycles may vary according to tissue type as well as limiting factors such as location to adjacent structures that may cause undesired thermal heating at the margins of the ablation zone. Cryoablation also has the ability to preserve the collagen network and overall cellular architecture of treated tissue, thereby eliminating extensive scarring within the target organ. It is therefore less likely to cause nontarget tissue damage in structures immediately adjacent to the treatment zone. Visualization of the "ice ball" within treated tissue at the time of ablation enables more effective monitoring of the expanding margins of the ablation zone and minimizes inadvertent damage to adjacent nontarget tissues. Unlike with heat ablation, treated tissue is not denatured, so the cells of the body are able to reabsorb dead tissue and there is no residual ablation "cavity. Further analysis of this technique by way of carefully designed randomized controlled trials is necessary to establish its efficacy relative to other more thoroughly studied thermal ablation modalities. Theoretical risks for bleeding and collateral damage to adjacent nontarget tissues exist, but risk of occurrence is unknown. Small observational studies published to date demonstrate low rates of major complications, comparable with other thermal ablation techniques. Risks for significant bleeding and damage to nontarget organs such as the colon may be minimized through use of laparoscopic or open surgical approaches, given the ability to mobilize adjacent critical organs and control bleeding if it occurs. Special diffusing applicators are mounted on the ends of optic fibers which are surrounded by protective glass domes. Manufacturers have developed applicators that use optic fibers of varying composition, length, and diameter to alter the size of the heated volume of tissue during the ablation procedure. Modifications to the applicator tip can also influence the distribution of scattered light within target tissue, thus altering the shape of the ablation zone. The technique involves percutaneous placement of multiple small needles under imaging guidance in to the target tissue lesion, through which a series of thin flexible optic fibers are inserted. A low-power laser energy source is then coupled to these optic fibers to deliver light energy to the target tissue, which in turn causes local heat deposition around the tips of the implanted optic fibers. Very high local tissue temperatures can be achieved, resulting in protein denaturation and cell death. Use of potentially flammable antiseptics, anesthetics, and medical gases should be avoided during the procedure. While sedated, patients undergo continuous monitoring with pulse oximetry and electrocardiography and blood pressure measurements are obtained at five-minute intervals during the ablation procedure. The procedure is performed under sterile technique, and the skin entry site must be appropriately cleansed and draped prior to intervention. Preliminary scout imaging confirms the size and location of the tumor to be ablated, and the optimal number and configuration of fiberoptic applicators to be placed is determined so as to achieve adequate coverage of the target lesion during ablation. Using imaging guidance, single or multiple thin cannulated puncture needles are percutaneously positioned within the target tissue lesion along a safe, pre-planned trajectory. Once appropriately positioned, the inner stylet of each needle is removed and exchanged for a 600-micron-diameter laser optic fiber. The needle is then partially withdrawn to expose the optic fiber tip within the target tissue. Similar to other thermal ablation modalities, internally cooled laser applicators are available to maximize the extent of heat deposition and coagulation necrosis within the ablation zone. In addition, lack of standardization regarding follow-up criteria by which to determine treatment success also makes interpretation of overall efficacy data difficult. Minor complications were more common and included asymptomatic pleural effusion, postprocedural fever, and severe pain in the immediate posttreatment period. Tumor seeding of the percutaneous laser fiber tracts is a very rare occurrence, and there were no reported cases in this study. Despite advancements in the design of thermal applicators, treatments are still inherently limited by heterogeneous heat convection profiles in hypervascular liver tissue. The potential therapeutic benefits that can be achieved through synergistic use of these therapies, however, cannot be understated.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.