
Zestoretic
General Information about Zestoretic
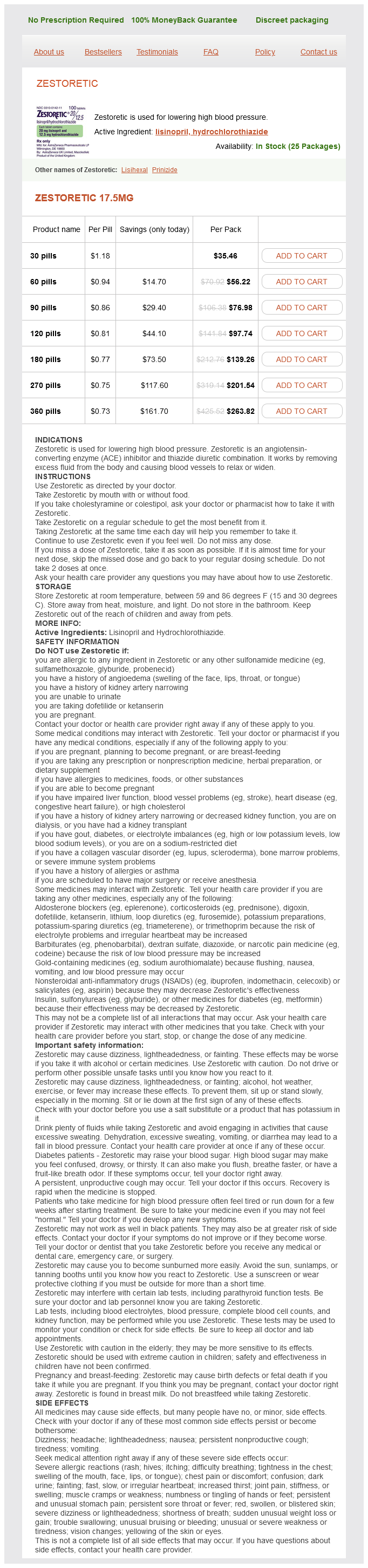
Zestoretic, additionally recognized by its generic name lisinopril-hydrochlorothiazide, is a commonly prescribed treatment used for the treatment of high blood pressure. This mixture drug accommodates two lively ingredients: lisinopril, an ACE inhibitor, and hydrochlorothiazide, a diuretic. Together, these two medications work to reduce back blood stress and forestall certain problems related to hypertension.
The different component of Zestoretic, hydrochlorothiazide, is a diuretic that works by increasing the quantity of water and salt expelled from the physique by way of urine. This in flip reduces the volume of fluid within the blood vessels, also reducing blood strain.
Zestoretic has been shown to successfully lower blood stress and is a crucial tool within the treatment of hypertension. However, it isn't an alternative selection to a wholesome way of life. A balanced food plan, common train, and stress management also can play important roles in managing blood stress. It is essential to proceed monitoring blood stress and make needed life-style changes along side taking Zestoretic to successfully manage hypertension.
High blood stress, also identified as hypertension, is a typical situation by which the force of blood against the artery partitions is constantly too high. Over time, this will cause injury to the blood vessels, coronary heart, and other organs. If left untreated, it might possibly enhance the chance of great well being problems such as coronary heart assault, stroke, and kidney illness. Zestoretic might help to lower blood stress and cut back the chance of these issues.
Zestoretic is often taken once a day, with or without meals. The dosage might vary depending on particular person wants and response to treatment. It is important to observe the prescribed dosage and proceed taking the treatment even if you feel well. Abruptly stopping Zestoretic could cause a sudden increase in blood stress, which could be dangerous.
Lisinopril, one of many lively ingredients in Zestoretic, works by blocking the manufacturing of angiotensin II, a hormone that causes blood vessels to constrict and slim. By inhibiting the action of this hormone, lisinopril permits blood vessels to relax and widen, which lowers blood strain. This helps to enhance blood move and scale back the workload on the heart.
In conclusion, Zestoretic is a combination medication used for the remedy of high blood pressure. Its mechanism of action includes relaxing blood vessels and decreasing fluid quantity to lower blood stress. While it's usually well-tolerated, potential unwanted effects and drug interactions ought to be considered. Zestoretic can be an essential device in managing hypertension, but should be used in conjunction with a healthy life-style for optimal outcomes. As always, it could be very important seek the guidance of your physician for any questions or concerns relating to your blood strain therapy plan.
As with any medication, there are potential unwanted effects associated with Zestoretic. Common unwanted aspect effects might embody dizziness, headache, fatigue, and dry cough. In some cases, extra serious unwanted side effects corresponding to allergic reactions, decreased kidney operate, and electrolyte imbalances might occur. It is important to report any regarding signs to your doctor immediately.
Before taking Zestoretic, you will need to inform your physician about any pre-existing conditions, allergy symptoms, and medicines you may be currently taking. This includes over-the-counter medication, nutritional vitamins, and supplements. Zestoretic might interact with other drugs, significantly non-steroidal anti-inflammatory drugs (NSAIDs) similar to ibuprofen, aspirin, and naproxen. It is also not really helpful to be used during pregnancy or whereas breastfeeding.
Increased signaling through receptors that control the activation of innate immune cell function lead to hyperresponsiveness to immune signals arrhythmia symptoms in children discount zestoretic. As the signaling abnormalities affect innate and adaptive immune cells, patients with these latter mutations often present with overlapping clinical features of autoinflammation, mild immunodeficiencies, and autoimmunity. The blockade of these respective amplification loops has become an effective therapeutic strategy. In many instances, a clinical diagnosis can be made on the basis of clinical features, which is then confirmed by genetic testing. Exon 10 has two mutational "hot spots" (M680 and M694) that have more than one known mutation. Attacks usually last for 24 to 72 hours, although arthritis can persist for up to 1 week. Physical exertion, emotional stress, and menses have been associated with attacks in some patients, but in many cases, there is no obvious provocation. Some patients experience a "prodromal sensation" for several hours before the onset of the attack, and chills often herald the onset of fever. Symptomatic nonuremic pericarditis is rare, but if present tamponade has been described. Familial Mediterranean fever arthritis often presents in childhood as monoarticular arthritis affecting the knee or ankle, with symmetric oligoarthritis being the next common presentation. The arthritis typically resolves completely without radiographic residua; however, before the colchicine era, untreated monoarticular arthritis of the hip often led to joint destruction necessitating joint replacement. Kidney amyloidosis presents with progressive proteinuria, nephrotic syndrome, and chronic renal failure. Rare side effects of colchicine include bone marrow suppression and a myoneuropathy that is most often seen in older adults with renal insufficiency. Safety assessments include regular measurements of blood counts and serum chemistries. The concomitant administration of oral and intravenous colchicine has been associated with fatal toxicity. Note the predominantly perivascular infiltrate with mixed, predominantly mononuclear cells (hematoxylin and eosin stain, ×1000). Other provocative factors include infections, emotional stress, trauma, and surgery, but in many instances, there is no obvious trigger. With increasing age, there is a tendency for the attacks to become less frequent and less severe. Unexplained adhesions are sometimes found, consistent with a history of peritoneal inflammation. Other dermatologic findings include erythematous papules and nodules, urticaria, annular erythema, and purpura. Because most patients have at least one copy of either the V377I or I268T mutation, these mutations have been used as a costeffective screening before undertaking more comprehensive sequencing. Corticosteroids may help to control attacks in some patients, but long-term toxicity is a major concern. However, important differences,100,101 including a much longer duration of attacks, migratory areas of erythema, swelling and myalgia, conjunctivitis and periorbital edema, poor response to colchicine, and a relatively prompt response to corticosteroids, suggested a different disease entity. The R92Q and P46L variants are seen in 1% to 4% of white and a 2% or higher percentage of African American, Arab, and sub-Saharan African populations 104-106 with similar frequencies in patients and the local populations. Although episodes sometimes develop with no apparent provocation, physical or emotional stress, physical trauma, and menses are sometimes associated with attacks; pregnancy may be associated with an amelioration of symptoms. A small minority of patients experience waxing and waning symptoms on a nearly daily basis. Symptomatic pericardial involvement is much less common than peritoneal or pleural inflammation. Typically, these occur as a localized area of cramping muscle pain, often with warmth and tenderness to palpation, and an overlying erythematous, blanchable rash, usually on the torso or the extremities. When it occurs on the limbs, the area of inflammation migrates centrifugally over the course of several days, probably along fascial planes, and is often associated with synovitis and effusion as it crosses a joint. Consistent with the normal muscle enzymes, a full-thickness biopsy in one patient demonstrated panniculitis, fasciitis, and perivascular inflammation but no involvement of the myofibrils themselves. Although these parameters may fluctuate with attacks, they often remain elevated even between attacks. Many patients exhibit anemia of chronic disease, polyclonal hypergammaglobulinemia, and low-titer IgM and IgG anticardiolipin antibodies. Corticosteroids can be used to treat the attacks, but patients frequently require escalating dosages, often with diminishing efficacy and serious toxicity. Endogenous triggers include "indicators of cellular injury," such as extracellular adenosine triphosphate; "indicators of metabolic stress," such as elevated extracellular glucose; and factors that lead to lysosomal damage, including crystalline/particulate matter. In contrast to familial and acquired cold urticaria, the result of the ice cube test is negative, and histologically, skin biopsies show a dermal polymorphonuclear perivascular infiltrate, which is distinct from the lymphocytic and eosinophilic infiltrate found in classical allergic urticaria. Other manifestations in mainly severely growth-retarded patients include soft, doughy palms, soles, fingers, and toes and clubbing of the fingernails in the absence of pulmonary disease. Sensorineural hearing loss caused by chronic inner ear inflammation typically develops in the second to third decade of life, but the onset and severity may vary with certain mutations149 and likely reflect the inflammatory organ damage of the Corti organ. Radiographs of the long bones indicate the location of epiphyseal lesions and are used to monitor the bony overgrowth and longitudinal bone growth and to determine the need for surgical interventions such as osteotomies and stapling of the growth plates. Furthermore, in patients with somatic mutation (see section on genetics and pathophysiology), the diagnosis of somatic mutations remains challenging.
Angiography blood pressure chart when to go to the hospital discount zestoretic 17.5 mg with visa, scintigraphy, intraosseous pressure, and histologic findings in high-risk osteonecrotic femoral heads with negative magnetic resonance images. F-18 fluoride positron emission tomography/computed tomography in the diagnosis of avascular necrosis of the femoral head: Comparison with magnetic resonance imaging. Spontaneous osteonecrosis of the knee: the result of subchondral insufficiency fracture. Spontaneous osteonecrosis of the knee: histopathological differences between early and progressive cases. The role of subchondral insufficiency fracture in rapid destruction of the hip joint: a preliminary report. The use of bisphosphonate in, the treatment of osteonecrosis of the femoral head: a meta-analysis of randomized control trials. Core decompression and conservative treatment for avascular necrosis of the femoral head: a meta-analysis. Long-term results of total hip arthroplasty for osteonecrosis of the femoral head. Transient osteoporosis of the hip in pregnancy: natural history of changes in bone mineral density. Idiopathic transient osteoporosis of the pelvis in a non-pregnant young woman: a case study. Rheumatoid manifestations of endocrine and lipid disease Cianna Leatherwood · Simon M. Helfgott Key Points Musculoskeletal abnormalities occur commonly in association with endocrine disease. Glandular dysfunction involving the adrenal, pituitary, pancreas, parathyroid, and thyroid may manifest as rheumatologic disorders. Nonspecific rheumatic manifestations and more characteristic abnormalities may occur. Muscle, tendon, bone, and joint abnormalities are more likely after periods of metabolic imbalance. Resolution or improvement of the clinical manifestations of rheumatic disease may occur on restoration of metabolic balance. Primary hyperlipidemias (hyperlipoproteinemias) result from abnormal metabolism of lipoproteins with an increase in their blood levels. Six types of hyperlipoproteinemias are recognized and differ on the basis of their lipoprotein profiles and musculoskeletal manifestations. Tendon xanthomas consist of lipid infiltrates, which result in irregular thickening of the involved tendon. During the repair mechanism, the regenerating fibrocartilage layer is excessive and forms a layer covering the old hyaline cartilage on the exposed bone. These structural alterations result in eburnation of subchondral bone and cyst formation that resembles severe forms of osteoarthritis. Joint effusions are uncommon; rarely, some patients may experience episodes of pseudogout. Physical examination shows evidence of bony enlargement and soft tissue prominence surrounding affected joints. Radiographs may show the hallmark features of acromegaly, namely widened joint spaces with chondrocalcinosis, osteophyte formation, and calcification of ligamentous insertions. Prognathism is commonly seen and usually accompanied by widening of the interdental spaces. Both types 1 and 2 diabetes mellitus are associated with a range of musculoskeletal and rheumatologic problems (Table 207. The condition of Dupuytren contracture consists of palmar and digital nodules and cords, palmar skin tethering, and digital contractures. In the early course of the disease, elevated growth hormone and insulin-like growth factor type I levels promote the growth of articular cartilage and periarticular ligaments, leading to cartilage thickening and joint space congestion. In this phase, joint space widening and periarticular soft tissue hypertrophy occur. Hyaline cartilage becomes thickened with clusters of large active basal chondrocytes; marginal osteophyte formation becomes excessive and periosteal fibrocartilaginous attachments hypertrophy and ossify. Despite frequent back pain, back mobility is maintained even with aging because the thickened intervertebral disk cartilage, together with lax hypertrophied paraspinal ligaments, contribute to increased spinal mobility. Metformin, a commonly used biguanide that works to inhibit gluconeogenesis and therefore decrease hepatic production of glucose, has been associated with myalgias. The mechanism is unknown but is potentially related to reduced levels of vitamin D. When compared with a nondiabetic population, trigger finger in patients with diabetes is more commonly seen in females and is more often bilateral and involves multiple digits with relative sparing of the index and small fingers. Over time, evidence of severe osteolysis may be seen, and bone and joint destruction may follow. The condition is sometimes self-limiting and one sided even though the neuropathy is permanent and symmetric. The condition is characterized by progressive muscle stiffness, rigidity, and spasm involving the axial muscles with severe impairment of ambulation. The hallmark feature is the presence of superimposed, severe episodic muscle spasm precipitated by sudden movement, noise, or emotional upset (startle reflex). Stiff person syndrome and type I diabetes share some immunologic features, including the presence of antibodies to glutamic acid decarboxylase, although the magnitude of the antibody response and the selected epitopes that are recognized differ in these two diseases. It most frequently occurs in one thigh muscle, but has been reported in the calves and upper extremities. Thyroid deficiency is more frequently associated with musculoskeletal symptoms than hyperthyroidism is. In older patients, hypothyroidism may mimic a polymyalgia rheumaticalike disorder consisting of proximal achiness around the shoulder and pelvic girdle muscles and generalized stiffness.
Zestoretic Dosage and Price
Zestoretic 17.5mg
- 30 pills - $35.46
- 60 pills - $56.22
- 90 pills - $76.98
- 120 pills - $97.74
- 180 pills - $139.26
- 270 pills - $201.54
- 360 pills - $263.82
In the United Kingdom pulse pressure 100 order genuine zestoretic on line, hip fracture rates are approximately 40% higher in women and 60% higher in men living in Scotland compared with those living in London. These fractures show a steep rise in incidence during the perimenopausal period in women but tend to plateau thereafter. A much stronger sex ratio exists for this fracture than for most others, estimated to be 4 to 1 in favor of women. Data from Dorset in the United Kingdom showed that in women, the incidence of distal forearm fracture rose from a premenopausal baseline of 10 per 10,000 of the population per year to a peak of 120 per 10,000 of the population per year older than 85 years. A winter peak is again demonstrated, but unlike hip fractures, this peak is probably due to falls outside on icy surfaces. The plateau with age in women may be due to the mode of falls because later in life a woman is more likely to fall onto a hip than onto an outstretched hand because of deterioration in neuromuscular coordination. In general, the presence of previous vertebral deformities has been shown to increase the risk for subsequent vertebral deformities by 7- to 10-fold. In a retrospective cohort study of 1288 residents of Rochester, Minnesota, a distal forearm fracture occurring when 35 years or older was associated with a 1. In contrast, a previous distal forearm fracture increased the risk for vertebral fracture across all ages, with a 5. This increased risk was more marked in patients with vertebral deformities associated with moderate or minimal trauma than with severe trauma. In the United States, data from the Study of Osteoporotic Fractures (a prospective study of 9704 U. In the United Kingdom, a study has recently shown that 25% of patients with a new low-trauma nonvertebral fracture had evidence of a previous vertebral fracture. Many of these factors remain poorly elucidated, but with improved understanding, it is hoped that novel public health measure may be identified. Until recently, accurate epidemiologic studies of vertebral fracture had been limited, partly because of the often asymptomatic nature of the fracture, as well as a lack of consensus regarding the techniques that should be used to define vertebral deformity. However, the advent of morphometric and semiquantitative visual techniques has now enabled a number of studies to report on the prevalence of vertebral deformity as a marker of vertebral osteoporosis and fractures. About one third of all vertebral fractures noted on radiographs come to medical attention, and fewer than 10% necessitate admission to a hospital. There is a threefold variation in the occurrence of deformity across Europe and up to a twofold variation in centers within individual countries, perhaps reflecting a combination of environmental and genetic factors. The risk for vertebral deformity in men was significantly elevated in those with high levels of physical activity, suggesting the importance of trauma (possibly occupational) as a cause. By contrast, women with higher levels of physical activity may have a reduced risk for deformity. For example, the risk for vertebral fractures in postmenopausal women in Beijing is only 25% lower than that in women in the United States despite much lower hip fracture rates in the former. In the United States, the cost of osteoporotic fractures in 2005 was estimated to be $19 billion. Expenditures are rising faster than the general rate of inflation and are a major source of concern to governmental leaders. Much research is currently focusing on the cost-effectiveness of treatment programs for osteoporosis. At present, this still remains difficult to assess, and the widespread use of expensive drugs may not be affordable in many countries. The world population is expected to increase from the current 323 million individuals 65 years or older to more than 1. These demographic changes alone can be expected to increase the number of hip fractures occurring worldwide. Likewise, in the United States, as the population older than 65 increases from 32 million in 1990 to 69 million in 2050, the number of hip fractures is expected to triple. In the United States in 2005, the total number of estimated incident fractures was higher than 2 million, with 72% of the cost being accounted for by hip fractures alone. By 2025, annual fractures and cost were predicted to rise by almost 50%, with the most rapid growth seen in the 65- to 74-year-old group (87% increase) and in Hispanic and other nonwhite subpopulations (175% increase). The impact of osteoporotic fractures is farreaching, not only for the individual but also for the health service, economy, and population as a whole. Osteoporotic fractures are expected to rise in subsequent generations because of an increase in life expectancy and a higher proportion of older individuals in most countries; however, rates have fallen in many Western countries, possibly as a result of improved public screening and treatment programs. Recently, several of the risk factors for this disease have been elucidated and models have been developed to allow more accurate assessment of fracture risk in patients so that preventive and therapeutic measures can be implemented appropriately. Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis. Ethnic and geographic variations in the epidemiology of childhood fractures in the United Kingdom. Familial resemblance of radial bone mass between premenopausal mothers and their college age daughters. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Hip Fracture Outcomes in People Aged Fifty and Over: Mortality, Service Use, Expenditures, and Long-Term Functional Impairment. Back pain, disability, and radiographic vertebral fracture in European woman: a prospective study. Fracture incidence and association with bone mineral density in elderly men and women: the Rotterdam study. Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures.

ADDII BIOTECH is proud to announce that the company's manufacturing facility located at Baddii, Himachal Pradesh has recently been approved by Food & Drug Authority of Ghana.
Our Manufacturing capability includes a wide range of therapeutic products covering almost every segment.
ADDII BIOTECH given our strong emphasis on product quality and services.